Pagsusuri ng Thorax at Baga, Breath Sounds, at Respiratory Patterns
Mahahalagang Punto
- Pinagsasama ng thorax assessment ang symptom interview, inspection, palpation, at auscultation.
- Ang chest symmetry, tracheal alignment, breathing effort, at trends ng respiratory pattern ay gumagabay sa acuity decisions.
- Ang adventitious sounds at lumalalang work of breathing ay maaaring magpahiwatig ng mabilis na decompensation.
- Maaaring lumitaw ang respiratory-rate at capnography changes bago bumaba ang oxygen saturation sa maagang deterioration.
Pisyopatolohiya
Nakasalalay ang epektibong respiration sa magkakaugnay na thoracic mechanics, airway patency, alveolar ventilation, at gas exchange. Ang structural o functional disruption ay nagpapabago sa airflow patterns at sa breath sounds na naipapasa sa chest wall. Ang thorax ay umaabot mula base ng leeg hanggang upper abdomen at nakaayos sa thoracic cage at thoracic cavity. Ang thoracic cage ay binubuo ng sternum, costal cartilages, at 12 pares ng tadyang na nakakabit sa likod sa T1-T12; pinoprotektahan ng balangkas na ito ang puso at baga habang pinapahintulutan ang ventilatory motion. Karaniwang inilalarawan ang rib groups bilang true ribs (1-7), false ribs (8-12), at floating ribs (11-12). Kasama sa sternum ang manubrium, body, at xiphoid process, na may clinically useful landmarks sa suprasternal notch, sternal angle, at second-rib attachment level para sa rib/intercostal counting.
Madalas na sumasalamin ang abnormal respiratory patterns sa systemic acid-base stress, neurologic dysregulation, fatigue, o lumalalang cardiopulmonary disease.
Klasipikasyon
- Assessment domains: Subjective respiratory history, thoracic inspection at palpation, breath-sound auscultation, at respiratory-pattern analysis.
- Thoracic-structure domain: Thoracic cage (sternum, ribs, costal cartilages, thoracic vertebrae) at organisasyon ng thoracic cavity na naglalaman ng puso at baga.
- Landmark domain: Midclavicular, anterior axillary, at midaxillary reference lines para sa localization sa exam at interventions.
- Breath-sound groups: Normal bronchial/bronchovesicular/vesicular sounds versus adventitious sounds.
- Adventitious categories: Fine/coarse crackles, rhonchi, wheeze, stridor, at pleural friction rub.
- Pattern abnormalities: Apnea, bradypnea, tachypnea, Cheyne-Stokes, Kussmaul, orthopnea, at agonal breathing.
- Special-voice maneuvers: Whisper pectoriloquy, egophony, at bronchophony ay maaaring sumuporta sa hinala ng consolidation/pleural process kapag abnormal na malinaw o nabago ang voice transmission.
- Normal breath-sound map: Bronchial (trachea/larynx, loud/high pitch, mas mahaba ang expiration), bronchovesicular (major bronchi malapit sa 1st-2nd interspaces, medium pitch na may inspiratory-expiratory pause), vesicular (peripheral lung fields, soft/lower pitch).
- Adventitious profile: Fine crackles (high-pitched inspiratory popping), coarse crackles (lower-pitched inspiratory wet sounds), rhonchi (low-pitched continuous sounds mula sa larger-airway narrowing/secretions), wheeze (high-pitched continuous sounds mula sa smaller-airway narrowing), stridor (inspiratory upper-airway obstruction), pleural rub (grating pleural-inflammation sound).
Pagsusuri sa Pag-aalaga
Pokus sa NCLEX
Unahin ang pagkilala sa respiratory distress at airway threat bago kumpletuhin ang full lower-acuity documentation.
- Suriin ang timing ng dyspnea, changes sa cough/sputum, tobacco o vaping exposure, at functional tolerance.
- I-quantify ang smoking burden gamit ang pack-years (packs/day na minultiply sa years smoked) at isama ang secondhand-smoke exposure context para sa pediatric at household risk analysis.
- Sa bedside reassessment, isama ang kasalukuyang oxygen-delivery setup at active respiratory treatments kapag ini-interpret ang effort at breath-sound changes.
- Isama ang current/past respiratory diagnoses, medication history, at family respiratory history sa focused subjective assessment.
- Isama ang nutrition-focused history kapag persistent ang respiratory symptoms: 24-hour food/fluid recall, restrictive-diet pattern, at food-insecurity barriers na maaaring magpalala ng pulmonary-risk burden.
- Tanungin kung gumagamit ang pasyente ng home respiratory support o monitoring equipment (halimbawa oxygen, CPAP/BiPAP, nebulizer, o peak-flow meter) at kung paano ito ginagamit.
- Isama ang age, sex, cultural/environmental context, at health-practice factors kapag ini-interpret ang reported symptoms.
- Sa dyspnea interview, itanong ang onset, trigger exposure (activity/dust/animals/food), exertion threshold, duration, relievers, at positional/nocturnal symptoms (orthopnea, pillow count, nighttime breathlessness).
- Kung severe ang shortness of breath o may kasamang chest pain, itigil ang routine interview at mag-escalate para sa emergency support.
- Sa cough interview, itanong ang sputum amount/color, hemoptysis, associated fever/chills/night sweats, symptom duration, triggers, at treatment response.
- I-quantify ang dyspnea gamit ang 0-10 patient-reported scale at i-trend ang serial scores bago at pagkatapos ng interventions.
- I-screen ang modifiable respiratory-risk practices sa health history, kabilang ang smoking/vaping, home o occupational pollution exposure, vaccine refusal, inactivity, high-weight pattern, at poor fruit-vegetable intake.
- I-inspect ang chest configuration at symmetry, tracheal midline, accessory-muscle use, retractions, at nasal flaring.
- Ituring ang bagong tracheal deviation bilang high-risk cue para sa unilateral volume loss o pleural-space pathology at agad na mag-escalate.
- I-inspect ang chest-wall contour abnormalities tulad ng pectus excavatum o pectus carinatum, at iugnay ito sa quality ng thoracic expansion.
- Sa inspection, ihambing ang anteroposterior at transverse diameter; ang expected adult AP:transverse ratio ay mga 1:2.
- Bilangin ang respiratory rate sa loob ng buong isang minuto at i-classify ang expected adult baseline bilang mga 12-20 breaths/min na may nonlabored regular rhythm.
- Gamitin ang resting SpO2 context kasama ng respiratory rate; ang expected adult resting saturation ay karaniwang mga 94-100%, habang ang values na mas mababa sa baseline (lalo na sa chronic COPD) ay nangangailangan ng trend-based interpretation at follow-up.
- Suriin ang depth at inspiratory-expiratory timing; sa quiet breathing karaniwang mas maikli ang inspiration kaysa expiration, habang sa active breathing maaaring lumapit sa 1:1.
- Gamitin ang surface landmarks (sternal angle/second rib at thoracic reference lines) upang tuloy-tuloy na ma-localize ang auscultation points at intercostal spaces.
- Gamitin nang pare-pareho ang thoracic reference lines para sa telemetry-lead placement at iba pang chest procedures na nangangailangan ng eksaktong anatomic localization.
- Suriin ang tripod positioning at kawalan ng kakayahang magsalita ng buong pangungusap bilang bedside respiratory-distress cues.
- Ituring ang prolonged expiration at tripod positioning bilang high-risk bedside findings na maaaring sumasalamin sa obstructive air-trapping o malaking respiratory effort.
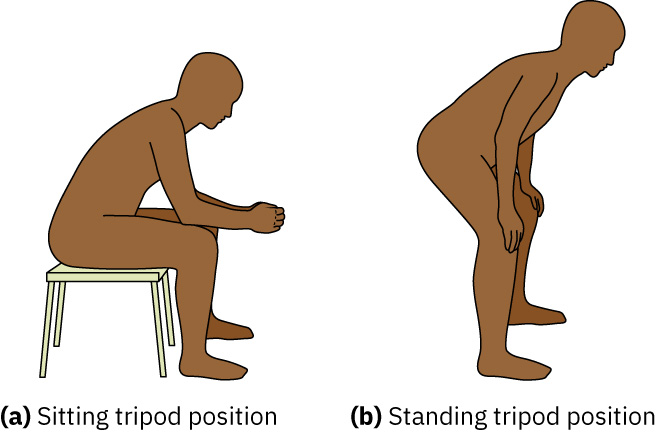 Illustration reference: OpenStax Clinical Nursing Skills Ch.23.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.23.2.
- I-inspect ang chronic hypoxia morphology tulad ng fingertip clubbing at increased anterior-posterior chest diameter (barrel chest); ang AP:transverse na malapit sa 1:1 ay sumusuporta sa hyperinflation patterns na madalas makita sa COPD.
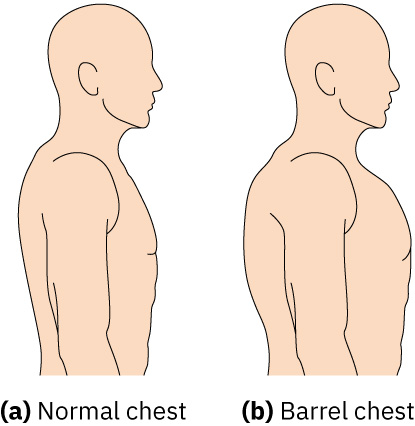 Illustration reference: OpenStax Clinical Nursing Skills Ch.23.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.23.2.
- I-inspect ang spinal posture (halimbawa kyphosis sa older adults) dahil maaaring baguhin ng thoracic-shape changes ang expansion patterns at breathing mechanics.
- I-characterize ang sputum ayon sa amount, color, odor, viscosity, at presence ng dugo; ang yellow/green purulent sputum ay sumusuporta sa infection-focused follow-up.
- Ituring ang rusty/brown sputum bilang posibleng lumang dugo at ang red/pink sputum (hemoptysis) bilang escalation cue na nangangailangan ng agarang clinical correlation.
- I-palpate para sa tenderness, masses, asymmetric expansion, at subcutaneous crepitus kapag indicated.
- Kung may napansing clavicular/chest-wall swelling pagkatapos ng recent airway instrumentation, i-palpate para sa subcutaneous emphysema (crepitus) at mag-escalate ng bagong findings.
- Pagkatapos ng chest-tube placement o removal, i-palpate malapit sa insertion site para sa crepitus o air-leak clues at mag-escalate ng bagong findings.
- Suriin ang symmetric chest expansion sa paglalagay ng kamay sa magkapantay na chest level at pag-obserba ng pantay na thumb movement habang humihinga.
- Ituring ang unequal unilateral expansion bilang abnormal cue para sa posibleng pneumonia o thoracic trauma (kabilang ang rib fracture o pneumothorax).
- Gumamit ng percussion upang ihiwalay ang expected lung-field resonance sa abnormal dullness na maaaring magpahiwatig ng consolidation o pleural-fluid accumulation.
- Mag-auscultate ng anterior at posterior lung fields nang sistematiko at ihambing ang side-to-side.
- Sa auscultation, ilagay ang stethoscope direkta sa balat (hindi sa ibabaw ng damit o buhok) at iwasan hangga’t maaari ang bony surfaces, clavicles/scapulae, at breast tissue.
- Gumamit ng upright position para sa pinakamahusay na sound transmission; kung hindi makaupo nang upright ang pasyente, ipihit sa magkabilang tagiliran sa kama at ipagpatuloy ang paired left-right comparisons.
- Gamitin ang diaphragm, i-coach ang deep mouth breathing, at makinig sa buong inspiratory-expiratory cycle sa bawat site.
- Kung pinaghihinalaan ang focal consolidation o pleural disease, magdagdag ng voice-transmission maneuvers (whisper pectoriloquy, egophony, bronchophony) at iugnay sa percussion at symptom findings.
- Mag-escalate nang mabilis kapag nagsama-sama ang distress signs: pursed-lip breathing, nasal flaring, audible breathing, intercostal retractions, anxiety, at accessory-muscle recruitment.
- I-evaluate ang breathing-pattern abnormalities sa clinical context: bradypnea (<12/min adult), tachypnea (>20/min adult), Cheyne-Stokes cyclical apnea-hyperventilation, Kussmaul deep rapid metabolic-acidosis pattern, orthopnea, dyspnea/PND, apnea, at agonal respirations.
- Sa older-adult trend interpretation, kilalanin na maaaring mangyari ang Cheyne-Stokes patterns nang walang acute pathology, pagkatapos ay iugnay sa oxygenation at neurologic findings bago escalation.
- Suriin ang medication-related respiratory cues sa history (halimbawa ACE inhibitor-associated dry cough o NSAID-sensitive bronchospasm patterns).
- Isama ang concurrent lung-assessment parameters: skin color (cyanosis/pallor), pleuritic pain, accessory-muscle use, at finger clubbing.
- Sa newborns at infants, bilangin ang respirations sa buong isang minuto habang kalmado ang bata; maaaring mangyari sa unang linggo ng buhay ang periodic breathing pauses hanggang mga 10 seconds at hindi ito abnormal maliban kung may distress signs.
- Para sa infants at young children, unahin ang maagang pagtukoy ng nasal flaring/retractions at isaalang-alang ang developmental mechanics (obligate nose breathing sa early infancy; AP:transverse na madalas malapit sa 1:1 hanggang mag-mature ang thoracic musculature around age six).
- Sa infants at young children, kunin mula sa caregivers ang subjective respiratory-history details kapag nililimitahan ng developmental stage ang direktang symptom reporting.
- Sa infants at young children, kilalaning maaaring relatively nonproductive ang cough at limitado ang respiratory-muscle endurance, kaya mabilis ang paglala ng secretion retention at fatigue.
- Sa preterm o ibang vulnerable neonates, panatilihin ang heightened surveillance para sa surfactant-related atelectatic patterns sa panahon ng respiratory illness.
- Sa pediatric respiratory illness, i-screen ang multisystem cues ng deterioration (decreased oral intake, fewer wet diapers/urine output, sunken fontanel sa infants, tachycardia, altered mentation, fatigue, cyanosis, at dry mucous membranes o poor skin turgor).
- Para sa older adults na may shallow breathing o respiratory-muscle fatigue, hatiin ang deep-breath auscultation sa mas maiikling segments na may rest periods (halimbawa anterior lung fields muna, pagkatapos posterior) upang mabawasan ang fatigue-related assessment error.
- Gamitin ang finding clusters upang paliitin ang malamang na komplikasyon: unilateral diminished sounds/expansion lag (atelectasis o pneumothorax), cough plus wheeze/URI history (bronchitis), crackles na may pink frothy sputum/peripheral edema (pulmonary edema), at diminished sounds na may pleuritic pain/fever (pleural effusion).
Mga Interbensyon sa Pag-aalaga
- Agarang mag-escalate ng increased work of breathing, severe pattern abnormalities, at bagong high-risk adventitious sounds.
- Iposisyon upang ma-optimize ang ventilation, suportahan ang oxygen therapy ayon sa orders, at bawasan ang exertional demand.
- Ilapat ang smoking-cessation Five As para sa mga pasyenteng handang tumigil: Ask, Advise, Assess readiness, Assist with counseling/pharmacotherapy, Arrange early follow-up.
- Muling suriin pagkatapos ng interventions at i-report ang objective trend changes sa effort, sounds, at oxygenation.
- I-monitor ang respiratory rate, rhythm, depth, at effort bilang tuloy-tuloy na trend data sa halip na isolated values.
- I-track ang chest movement symmetry, accessory-muscle use, at intercostal o supraclavicular retractions.
- Mag-auscultate para sa decreased o absent ventilation at adventitious sounds, pagkatapos ay i-map ang changes ayon sa lokasyon at severity.
- Gumamit ng oxygen-saturation monitoring na may angkop na alarms sa clients na may panganib sa hypoxia ayon sa policy.
- Gumamit ng ABG data kapag indicated para sa severe compromise, at tandaan na invasive ang test at dapat i-interpret kasabay ng bedside trends.
- Sa sedated clients, unahin ang continuous pulse-oximetry trend monitoring at agarang alarm response.
- Ipagpatuloy ang close trend monitoring kahit matapos ang short-term oxygen-saturation improvement dahil maaaring mabilis na bumalik ang acute respiratory distress.
- Sa adults na walang chronic low baseline, mag-escalate ng bagong SpO2 na mas mababa sa 92%; ituring ang SpO2 na mas mababa sa 88% bilang severe hypoxia na nangangailangan ng urgent intervention.
- Kung sabay lumitaw ang rapid shallow breathing, crackles, at reduced air movement, agad mag-escalate para sa urgent imaging at treatment ng posibleng severe pulmonary infection.
- Ituring ang bagong chest pain na may respiratory decline, o lumalalang dyspnea na may irritability/restlessness/LOC change, bilang immediate escalation findings.
- I-evaluate ang suctioning need sa pag-uugnay ng coarse airway sounds (rhonchi) sa secretion burden at cough effectiveness.
- I-monitor ang hypoxia progression cues tulad ng restlessness, anxiety, at air hunger.
- Isama ang bagong confusion o LOC change sa early hypoxia cue surveillance.
- I-dokumento ang onset, duration, at characteristics ng cough, kasama ang amount at quality ng secretions.
- I-track ang dyspnea triggers/relievers at isama ang chest-imaging findings sa longitudinal respiratory surveillance.
- Isama ang chest X-ray findings sa trend review at i-verify ang pregnancy status bago imaging escalation ayon sa policy.
- Kapag hindi malinaw ang escalation workup, asahan ang expanded respiratory diagnostics tulad ng CT/MRI, V/Q scan, o pulmonary-function testing ayon sa clinical context.
- Kung may chest pain na may pressure quality, jaw/arm radiation, dyspnea, dizziness, o nausea, mag-escalate bilang emergency bago ang routine focused pain workup.
- I-modify ang planned interventions ayon sa kasalukuyang dyspnea severity; kung lumalala ang distress, ihinto ang exertional tasks (halimbawa ambulation) at mag-escalate para sa RT consult o medication adjustment ayon sa orders.
- I-dokumento ang intervention effectiveness gamit ang reassessment trends sa heart rate, respiratory rate, pulse oximetry, lung sounds, at patient-reported dyspnea score.
- I-dokumento ang baseline at reassessment sa kumpletong lung-assessment format: respiratory symptoms/history, thorax symmetry at AP:transverse ratio, respiratory rate/effort/pattern, retractions o accessory-muscle use, palpation findings, bilateral auscultation map, at room-air o oxygen-supported SpO2.
Panganib ng Respiratory Failure
Ang retractions, stridor, agonal pattern, o mabilis na lumalalang dyspnea ay emergency findings na nangangailangan ng agarang escalation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| [bronchodilators] | Short-acting and long-acting agents | I-evaluate ang post-treatment breath-sound at work-of-breathing response. |
| [antibiotics] | Bacterial respiratory infection contexts | Iugnay ang regimen effectiveness sa fever, sputum, at auscultation trends. |
Aplikasyon ng Clinical Judgment
Clinical Scenario
Ang isang pasyenteng may COPD ay nagkaroon ng tachypnea, intercostal retractions, at bagong diffuse wheezing.
- Recognize Cues: Tumaas na respiratory effort na may bagong adventitious findings.
- Analyze Cues: Lumalala ang airflow limitation at maaaring umusad sa respiratory failure.
- Prioritize Hypotheses: Agarang prayoridad ang oxygenation at ventilation support.
- Generate Solutions: Simulan ang escalation, i-optimize ang positioning, at ihanda ang ordered respiratory interventions.
- Take Action: Ipaabot ang objective findings at bantayang mabuti ang trend response.
- Evaluate Outcomes: Bumubuti ang work of breathing at breath sounds pagkatapos ng treatment.
Mga Kaugnay na Konsepto
- respiratory system - Core anatomy at gas-exchange framework para sa focused respiratory assessment.
- pulmonary function testing at PEFR zones - Sumusuporta sa trend interpretation ng obstructive respiratory changes.
- oxygen therapy device selection at monitoring - Device selection at reassessment principles sa respiratory decline.
- documenting at reporting data - Pinapahusay ng objective pattern documentation ang kalidad ng escalation.
Sariling Pagsusuri
- Aling assessment findings ang nagpapahiwatig ng agarang respiratory escalation?
- Paano nakatutulong ang adventitious sounds sa pagliit ng posibleng pathophysiology?
- Bakit kailangang i-trend ang respiratory-pattern changes sa halip na ituring na isolated findings?