Pangkalahatang-ideya ng Shock
Mahahalagang Punto
- Ang shock ay estado ng hindi sapat na cellular/tissue perfusion na nagbabanta sa organ function at survival.
- Sa maagang shock, naa-activate ang sympathetic compensation (vasoconstriction, tachycardia, stress-hormone release), ngunit ang persistent hypoperfusion ay humahantong sa tissue hypoxia at cell death.
- Kabilang sa mga uri ang cardiogenic, hypovolemic, septic, at neurogenic pathways, na may magkakaibang sanhi ngunit iisang endpoint ng perfusion failure.
- Kritikal ang maagang pagkilala at intervention bago umusad sa irreversible stages.
Patopisyolohiya
Nangangailangan ang sapat na perfusion ng magkakaugnay na cardiovascular pump function, vascular tone, oxygen delivery, at end-organ regulation. Sa shock, binabawasan ng circulatory dysfunction ang tissue oxygen delivery. Lalong vulnerable ang cardiac output (CO = stroke volume x heart rate) kapag hindi kanais-nais ang preload, afterload, o contractility. Pinapataas ng compensatory sympathetic activation ang catecholamines at cortisol, na nagdudulot ng:
- Pagtaas ng heart rate
- Peripheral vasoconstriction
- Pansamantalang blood-pressure support
- Pagtaas ng circulating glucose para sa stress-energy demand
Kapag bumigo ang compensation, tumataas ang tissue oxygen debt, dumadami ang anaerobic metabolism, at naiipon ang lactic acid. Ang persistent severe tachycardia ay maaaring kalaunang magpababa ng ventricular filling at magpalala ng epektibong output. Ang tuloy-tuloy na hypoperfusion ay humahantong sa organ dysfunction at kalaunang cell death.
Hemodynamic Monitoring
Tumutulong ang hemodynamic monitoring upang masuri ang perfusion status at tugon sa therapy.
| Parameter | Typical reference | Shock pattern |
|---|---|---|
| Cardiac output (CO) | Humigit-kumulang 4-8 L/min | Bumababa sa low-output states |
| Cardiac index (CI) | Humigit-kumulang 2.5-4.0 L/min/m² | Madalas na mababa kapag hindi sapat ang perfusion |
| Stroke volume (SV) | Humigit-kumulang 60-100 mL/beat | Madalas na mababa sa pump-failure o preload-deficit states |
| Mean arterial pressure (MAP) | Humigit-kumulang 70-100 mmHg | Bumababa; perfusion concern kapag <65 mmHg |
| Central venous pressure (CVP) | Humigit-kumulang 2-6 mmHg | Madalas na mababa sa volume-loss states; maaaring tumaas sa piling obstructive/cardiogenic states |
| Pulmonary artery pressure (PAP) | Humigit-kumulang 11-20 mmHg (rest) | Maaaring tumaas sa pulmonary vascular o left-sided cardiac dysfunction |
| Pulmonary artery occlusion pressure (PAOP/wedge) | Humigit-kumulang 8-12 mmHg | Maaaring tumaas sa left-sided filling-pressure overload |
| Systemic vascular resistance (SVR) | Humigit-kumulang 800-1200 dynes/sec/cm⁻⁵ | Mababa sa distributive states at mataas sa vasoconstrictive states |
- Noninvasive assessment: pulse, blood pressure, capillary refill, skin temperature, edema pattern.
- Invasive assessment: arterial-line MAP at central-access pressure monitoring kapag kailangan ng tuloy-tuloy na high-acuity trends.
- Ang advanced invasive assessment sa piling ICU patients ay maaaring kabilang ang pulmonary-artery-catheter data upang pinohin ang low-output versus vasomotor shock interpretation.
- I-interpret ang hemodynamic variables bilang profile (pump, preload, at afterload) sa halip na hiwa-hiwalay na numero.
Mga Yugto ng Shock
Initial Stage
- Nagsisimulang bumaba ang cellular perfusion.
- Nagsisimula ang SNS activation, ngunit maaaring banayad pa ang mga overt clinical findings.
- Karaniwang maagang cues: banayad na agitation, bahagyang pagbaba ng urine output, at normal-to-slightly elevated vital signs.
Compensatory Stage
- Nagsisimulang bumaba ang blood pressure at tumitindi ang compensatory reflexes.
- Sinisikap ng baroreceptor-mediated sympathetic drive na mapanatili ang perfusion pressure.
- Ang catecholamine surge (norepinephrine/epinephrine) ay nagpapataas ng vascular tone at heart rate; nire-redistribute ang blood flow papunta sa utak at puso.
- Ang RAAS activation ay nagpapataas ng sodium-water retention at vasoconstriction, na nagbibigay ng pansamantalang blood-pressure support.
- Mas nagiging halata ang clinical deterioration kapag hindi naibabalik ang perfusion.
- Karaniwang compensatory-stage findings: mababang blood pressure, tachycardia, cool skin, nabawasang urine output, at normal-to-slightly elevated respiratory rate.
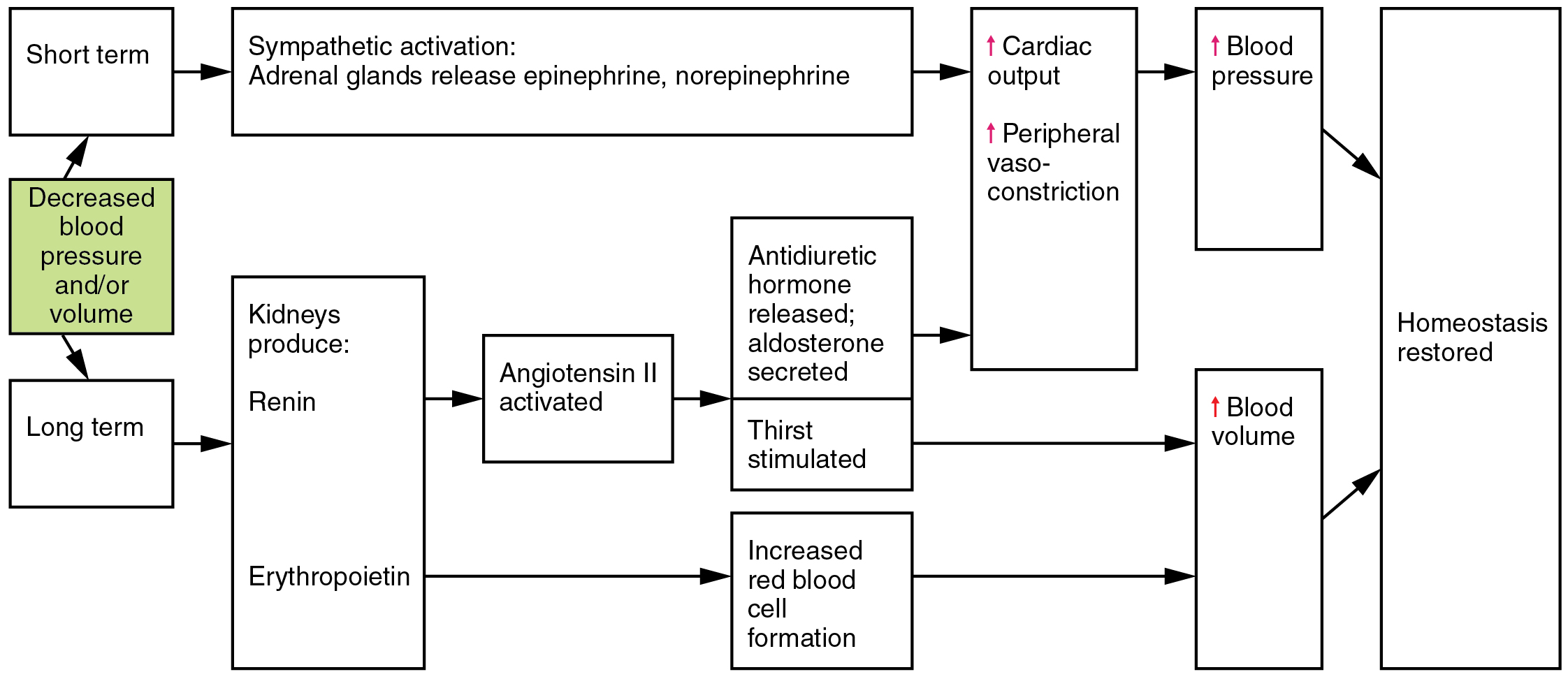 Illustration reference: OpenRN Health Alterations Ch.5.2.
Illustration reference: OpenRN Health Alterations Ch.5.2.
Maagang Organ-Level Consequences Habang Compensating
- Ang renal hypoperfusion ay nagtutulak ng renin release at fluid-conserving endocrine response.
- Ang tuloy-tuloy na pulmonary endothelial injury ay maaaring magpataas ng alveolar-capillary permeability, na nagdudulot ng pulmonary edema.
- Ang respiratory compromise ay maaaring umusad sa acute respiratory distress syndrome (ARDS) sa severe/decompensating pathways.
Progressive Stage
- Lalong bumababa ang cellular perfusion at kapansin-pansing tumataas ang capillary permeability.
- Tumatagas ang protein at fluid mula intravascular space papunta sa interstitial space, na nagpapalala ng effective circulating volume.
- Pinapabilis ng capillary-leak pattern na ito ang tissue hypoperfusion at itinataguyod ang pag-usad ng multi-organ dysfunction.
- Kabilang sa karaniwang progressive-stage cues ang lumalalang hypotension/tachycardia/tachypnea, cool clammy skin, mahihinang distal pulses, at pagbaba ng urine output.
- Ang tuloy-tuloy na hypoxia ay maaaring magdulot ng metabolic acidosis at dysrhythmia/ischemic cardiac complications.
Refractory Stage
- Nanatili ang malalim na hypotension at cellular failure sa kabila ng paggamot.
- Nagpapatuloy ang anaerobic metabolism, lactic acidosis, at severe capillary leak na may limitadong reversibility.
- Kadalasang findings: mottled skin, halos anuric na urine output, weak-to-absent peripheral pulses, at severe end-organ failure.
Pattern ng Organ-System Deterioration sa Progressive/Refractory Shock
- Cardiovascular: tachydysrhythmias, myocardial ischemia/infarction, panganib ng circulatory collapse.
- Pulmonary: pulmonary edema, impaired gas exchange, tumataas na work of breathing, ARDS progression.
- Neurologic: altered level of consciousness mula sa cerebral hypoperfusion.
- Renal: madalas na urine output na mas mababa sa 30 mL/hour na may tumataas na BUN/creatinine.
- Gastrointestinal/hepatic: barrier injury, mahinang nutrient absorption, jaundice, tumataas na liver-injury markers.
- Vascular/skin: third spacing, peripheral edema, pallor o cool clammy/mottled skin.
- Metabolic: electrolyte imbalance at metabolic acidosis.
Stage-Based Vital Sign Pattern
| Stage | Blood pressure | Heart rate | Respiratory rate | Urine output | Temperature | Skin/pulses |
|---|---|---|---|---|---|---|
| Initial | Normal hanggang bahagyang mataas | Normal hanggang bahagyang mataas | Kadalasang halos normal | Posibleng banayad na pagbaba | Karaniwang normal | Maaaring banayad pa ang maagang perfusion change |
| Compensatory | Mababa | Mataas | Normal hanggang bahagyang mataas | Nabawasan | Karaniwang normal | Cool skin, perfusion redistribution |
| Progressive | Mababa | Mataas | Mataas | Mababa | Madalas mababa | Cool clammy skin, mahihinang distal pulses |
| Refractory | Patuloy na mababa kahit may treatment | Markedly elevated | Elevated | Mababa hanggang halos zero | Mababa | Mottled cool skin, weak/absent peripheral pulses |
Panganib ng Multiorgan Dysfunction
Ang matagal na shock ay maaaring umusad sa multiorgan dysfunction syndrome (MODS). Mas mataas ang panganib sa older adults at mga pasyenteng may maraming comorbidities, lalo na sa severe hypovolemic o septic pathways.
Nursing Assessment
- I-track ang mental-status changes, urine output, skin perfusion cues, at vital-sign trends.
- I-interpret ang blood pressure sa konteksto ng perfusion; unahin ang MAP trend kaysa iisang single values lamang.
- Tukuyin ang maagang pag-usad mula banayad na compensation tungo sa decompensation.
- Mabilis na mag-escalate para sa persistent hypotension, lumalalang perfusion, o tumataas na organ-dysfunction indicators.
Nursing Interventions
- Suportahan ang mabilis na cause-directed stabilization ayon sa protocol at provider orders.
- Tiyakin ang madalas na reassessment ng perfusion indicators at hemodynamic trends.
- I-coordinate ang oxygenation, fluid, at vasoactive-therapy readiness sa high-risk patients.
- Sa refractory low-output cardiogenic pathways, asahan ang temporary mechanical-circulatory support escalation (halimbawa intra-aortic-balloon-pump counterpulsation) na may mahigpit na bleeding at distal neurovascular checks.
- Sa refractory cardiopulmonary failure, maghanda para sa extracorporeal-membrane-oxygenation escalation at i-monitor ang major complication domains (bleeding, thrombosis, infection, at limb ischemia) na may interdisciplinary coordination.
- Maagang ipabatid ang trend deterioration upang maiwasan ang pag-usad sa irreversible shock stages.
Paglalapat ng Clinical Judgment
Klinikal na Sitwasyon
Ang pasyente ay nagkaroon ng tumataas na heart rate, bagong agitation, cool extremities, at MAP na nagte-trend mula 74 tungo sa 66 mmHg sa loob ng 1 hour.
- Recognize Cues: Tachycardia, mental-status change, cool skin, bumababang MAP.
- Analyze Cues: Hindi na napapanatili ng compensatory physiology ang sapat na tissue perfusion.
- Prioritize Hypotheses: Ang nalalapit na pag-usad ng shock ang agarang banta.
- Generate Solutions: I-escalate ang monitoring intensity, ihanda ang rapid stabilization orders, at muling tasahin ang perfusion targets.
- Take Action: I-activate ang high-acuity response workflow, kumuha ng serial perfusion data, at suportahan ang inutusang interventions.
- Evaluate Outcomes: Bumubuti ang MAP at urine output, nagsi-stabilize ang mental status, at bumabawi ang end-organ perfusion signs.
Mga Kaugnay na Konsepto
- hypovolemic shock - Volume-loss shock pathway na may source-control at rapid-resuscitation priorities.
- cardiogenic shock - Low-output pump-failure phenotype na nangangailangan ng vasoactive at mechanical-support escalation.
- sepsis - Ang septic pathways ay maaaring umusad sa distributive shock at multi-organ dysfunction.
- sistemang cardiovascular - Sentral sa shock determinants ang pump function at vascular tone.
- mga vital sign indicator ng physiologic functioning at homeostasis - Mahalaga ang trend interpretation sa maagang shock recognition.
- mga indikasyon ng CVAD at pagpili ng device - Sinusuportahan ng central access ang invasive hemodynamic monitoring sa unstable states.
Sariling Pagsusuri
- Bakit maaaring mas kapaki-pakinabang ang MAP kaysa isolated systolic pressure sa shock monitoring?
- Aling mga maagang cue ang nagpapahiwatig ng paglipat mula initial tungo sa compensatory shock?
- Aling trend pattern ang dapat mag-trigger ng agarang escalation kahit bago lumitaw ang severe hypotension?