General Survey at Anthropometric Measurement sa Initial Assessment
Mahahalagang Punto
- Nagsisimula ang initial assessment sa structured general survey bago ang focused examination.
- Nagbibigay ang anthropometric measures ng objective baseline data para sa nutrition, risk stratification, at trend monitoring.
- Sa bedside inpatient workflows, kasama sa general survey ang height, weight, appearance, hygiene, behavior, at full vital signs upang magtatag ng shift/admission baseline.
- Nagsisimula ang general survey sa first contact at kabilang ang environmental sensory cues (ano ang nakikita, naririnig, nararamdaman, at naaamoy ng nurse).
- Maaaring magbunyag ang behavior at communication cues ng maagang hypoxia, neurologic deterioration, psychiatric distress, o pain-related instability.
- Dapat gabayan ng initial visual inspection findings kung kailan kailangan ang focused palpation o mas malalim na exam techniques.
- Direktang nakaaapekto ang observation quality at measurement technique sa mga susunod na clinical decisions.
- Dapat mag-trigger ang unexpected findings ng focused reassessment at escalation kapag clinically significant.
Pisyopatolohiya
Sinasalamin ng general survey findings ang integrated function sa neurologic, respiratory, cardiovascular, metabolic, at behavioral systems. Ang mga pagbabago sa appearance, mobility, speech, posture, o distress cues ay maaaring maagang palatandaan ng instability bago pa lumitaw ang laboratory o imaging abnormalities.
Ang anthropometric trends (halimbawa height/weight pattern shifts) ay maaaring magpahiwatig ng fluid imbalance, malnutrition, chronic disease progression, o treatment effects. Sinusuportahan ng tumpak na baseline measurement ang makabuluhang paghahambing sa paglipas ng panahon.
Klasipikasyon
- General survey domains: Appearance, behavior, level of distress, body position, gait/mobility, hygiene, at communication cues.
- General-survey continuity domain: Nagsisimula sa first contact at nagpapatuloy sa buong care interactions habang may lumalabas na bagong cues.
- First-impression cue domains: Environmental safety/comfort, interaction quality, verbal at nonverbal communication, at observable respiratory effort.
- Physical-exam technique domain: Kabilang sa objective assessment methods ang inspection, auscultation, palpation, at percussion.
- Anthropometric domains: Height, weight, BMI-related interpretation, at trend direction sa paglipas ng panahon.
- Extended anthropometric domains: Waist/hip/limb circumference, pediatric head/chest circumference trends, at selected body-composition proxies.
- Anthropometric device matching: Standing, bed, sling, at bariatric scale options na pinipili ayon sa mobility status at safety requirements.
- Developmental domains: Age-expected gross/fine motor, speech/language, at social milestones.
- Cognitive-status domains: Orientation (person/place/date/time), level of consciousness terms, at structured tools tulad ng GCS kapag indikado.
- Cognitive follow-up tools: Focused neurologic screening, targeted medication/substance-history questions, at structured tools (halimbawa MMSE) kapag abnormal ang screening.
- Instrument domains: Vital-sign tools (thermometer, stethoscope, BP cuff, pulse oximeter) at anthropometric tools (scale, height device, tape, calipers).
- BMI stratification: Underweight (<18.5), healthy range (18.5-24.9), overweight (25-29.9), obesity (>=30.0), at severe obesity (>=40.0).
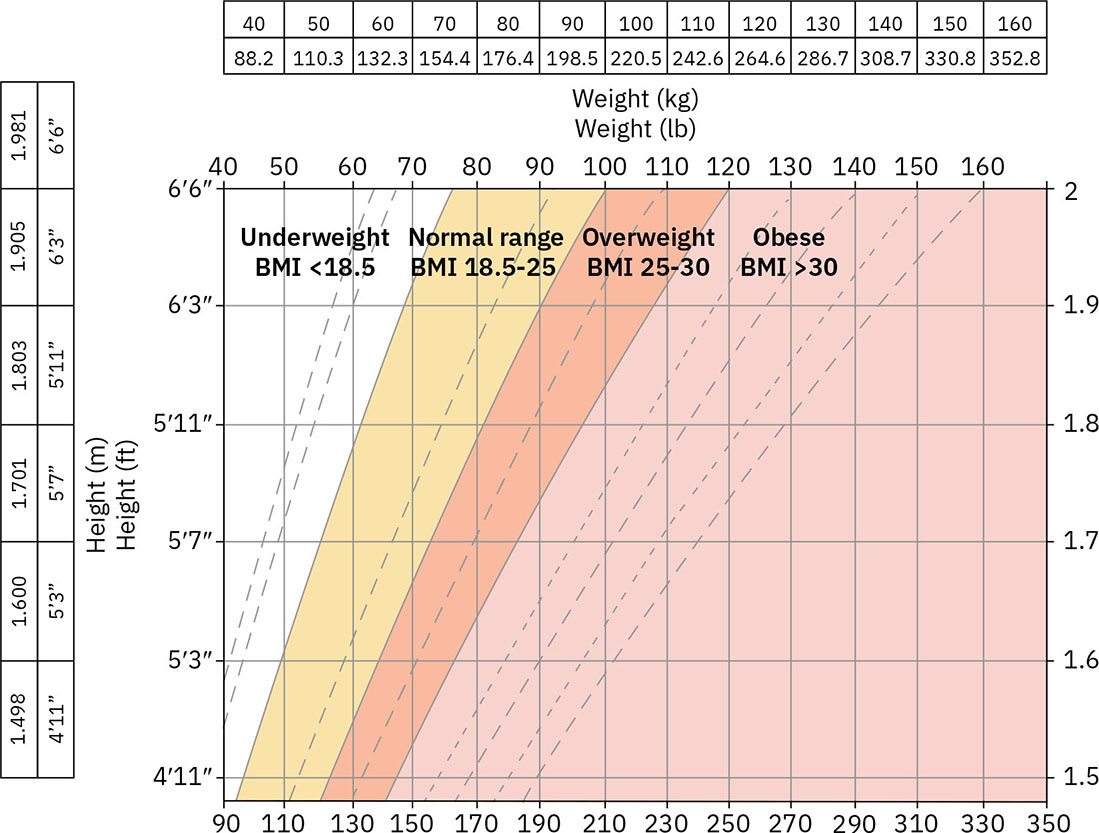 Illustration reference: OpenStax Clinical Nursing Skills Ch.15.
Illustration reference: OpenStax Clinical Nursing Skills Ch.15. - BMI interpretation limits: Screening tool ang BMI at maaaring magkamali sa pag-classify ng adiposity sa clients na may mataas na muscle mass, atypical body composition, at population-specific fat-distribution differences.
- BMI age context: Karaniwang inilalapat ang routine BMI computation mula humigit-kumulang age 2 pataas na may age-appropriate interpretation sa pediatrics.
- Clinical-use class: Baseline establishment, risk detection, at response-to-treatment monitoring.
Pagsusuri sa Pag-aalaga
Pokus sa NCLEX
I-prioritize ang objective cue capture at trend reliability bago magbuo ng konklusyon mula sa isang isolated value.
- Isagawa ang first-look assessment nang sistematiko at idokumento ang objective descriptors sa halip na assumptions.
- Isama nang maaga ang room at context observations (temperature, noise level, unusual odors, clutter/safety concerns).
- Kumuha ng anthropometric measures gamit ang standardized technique at calibrated equipment.
- Kumpirmahin ang unit consistency at conversion accuracy kapag nagdodokumento o nagtuturo (kg/lb at cm/in).
- Ikumpara ang findings sa age/context expectations at kilalang baseline data.
- Itakda ang monitoring frequency ayon sa clinical context (single baseline sa admission kumpara sa daily/weekly trend surveillance).
- Suriin ang speech clarity, pace, at emotional tone sa interaction; ang garbled o slurred speech ay nangangailangan ng focused neurologic follow-up.
- Suriin ang response sa simpleng commands dahil maaaring magpahiwatig ng acute cognitive o neurologic change ang nabawasang comprehension o cooperation.
- Suriin nang maaga ang language-access needs at i-activate ang qualified interpreter support kapag may language discordance.
- Suriin ang communication-accommodation needs sa first contact (halimbawa interpreter pathway, hearing-aid availability, o iba pang assistive communication supports).
- Suriin ang behavior patterns para sa urgency cues: restlessness, inability to remain still, lethargy, respiratory posturing, accessory-muscle use, o bagong inability to ambulate.
- I-reconcile ang verbal report sa nonverbal cues (halimbawa sinasabing “no pain” habang grimacing/guarding) bago isara ang assessment conclusions.
- Ihiwalay ang mood mula sa affect at idokumento ang incongruence (halimbawa flat affect o unexpectedly elated behavior sa high-risk contexts) para sa focused mental-status follow-up.
- Maingat na i-interpret ang eye contact patterns dahil maaaring baguhin ng cultural norms ang inaasahang nonverbal behavior.
- Suriin ang contextual modifiers (family history, metabolic factors, activity pattern) bago i-label ang obesity risk mula sa BMI lamang.
- Obserbahan ang family interaction patterns kapag may caregivers dahil maaaring baguhin ng role strain o conflict ang care participation at ADL support reliability.
- Suriin ang abuse indicators (fearfulness, withdrawal, unexplained bruises/burns, inconsistent explanations) at kumpirmahin ang safety concerns sa private interviewing kung posible.
- Suriin ang posibleng substance-use cues (halimbawa sobrang constricted o dilated pupils na may atypical behavior) at mag-escalate para sa focused evaluation.
- Magtanong nang direkta sa halip na mag-assume ng biological sex o cultural preferences; isama ang responses sa individualized assessment planning.
- Gumamit ng adjunct obesity-risk data kapag kailangan (diet pattern analysis, activity level, at iba pang body-composition assessments).
- Tukuyin ang red flags (rapid weight change, visible distress, altered mentation, severe fatigue, unstable mobility).
- Tayahin ang skin at mucous findings para sa concerning patterns: pallor, jaundice, cyanosis, flushing, abnormal moisture, at localized discoloration.
- I-prioritize ang high-risk skin color cues sa lips, mucous membranes, at sclera.
- Mag-screen ng fluid-status visual cues: dehydration patterns (dry skin, dry mucous membranes, sunken eyes) at fluid-overload patterns (peripheral edema na may bagong breathing difficulty).
- Sa infants, ituring ang sunken fontanel na may dry mucosa/skin bilang high-priority dehydration cue na nangangailangan ng focused reassessment.
- Sa pediatric assessments, isama ang head circumference hanggang early childhood at i-screen ang developmental progression kapag delayed o regressing ang milestones.
- Sa pediatric general-survey encounters, gumamit ng calm/gentle communication at demonstration sa dolls o stuffed animals kapag nililimitahan ng procedural fear ang cooperation.
- Sa pediatric physical exams, idokumento ang caregiver/chaperone presence at chaperone identity para sa sensitive breast/genital/anorectal assessment, habang iginagalang ang adolescent client comfort at chaperone-gender preference kung posible.
- Sa adolescent assessments, isama ang private interview time para sa sensitive risk topics bukod sa caregiver-present history.
- Idokumento ang orientation bilang A&O x4 (person/place/date o day/time context) at tandaan ang developmentally expected limits para sa infants/young children.
- Kung reduced ang consciousness, i-classify ang response level (halimbawa lethargic/obtunded/comatose) at ilapat ang structured LOC scoring kapag indikado.
- Kung abnormal ang screening cognition, palawakin ang assessment gamit ang focused neurologic/mental-status follow-up (halimbawa cranial nerve checks at MMSE-style tasks).
- Sa older-adult encounters, tiyaking nakasuot ang glasses/hearing aids, maglaan ng dagdag na response time, at gumamit ng collateral history sources kapag limitado ang direct communication.
- Agarang i-escalate ang sudden facial asymmetry o speech change bilang posibleng stroke cues.
Mga Interbensyon sa Pag-aalaga
- Gumamit ng reproducible measurement workflow (timing, device, positioning, documentation fields).
- Simulan ang encounters sa privacy setup, role-purpose-time explanation, at two-identifier verification (name/DOB kasama ang approved secondary verification source).
- Ulitin ang surprising values at kumpirmahin ang method accuracy bago mag-escalate.
- Tiyaking angkop ang sukat ng equipment at tugma sa age/body habitus upang maprotektahan ang measurement validity.
- Isama ang circumference measures kapag indikado: pediatric serial head/chest growth tracking at adult waist-centered adiposity risk assessment.
- Bago simulan ang survey observations, tugunan ang immediate readiness needs (halimbawa pain, toileting, at sensory aids) at lumihis sa emergency workflow kung may acute distress signs (halimbawa chest pain o breathing difficulty).
- Kung ang first-contact cues ay nagmumungkahi ng functional limitation (poor grooming, inappropriate dress, mobility difficulty), palawakin ang assessment para sa ADL at support needs.
- Gamitin ang inspection findings upang gabayan ang focused palpation at iba pang exam components kapag kailangan ng paglilinaw sa abnormalities.
- Gumamit ng active listening kasama ang adaptive follow-up questions kapag may off-script concerns ang pasyente na maaaring indikasyon ng hidden deterioration.
- Kung lumihis sa inaasahang trajectory ang growth o developmental findings, simulan ang focused endocrine/neurologic at functional assessment pathways.
- I-trigger ang focused assessments at provider notification kapag ang survey o measurement cues ay nagmumungkahi ng deterioration.
- Agarang i-escalate para sa critical-condition clusters: bagong unresponsive/altered mentation, breathing difficulty, out-of-range vital signs, o cool clammy cyanotic skin.
- I-chart ang general-survey findings bilang expected-versus-unexpected objective statements (appearance, orientation, speech/command response, mobility/posture, skin-mucosa, anthropometrics, at full vital-sign set na may oxygen context).
- Idokumento ang communication-support actions na ginamit sa bedside assessment (halimbawa interpreter use o hearing-assist setup) upang suportahan ang continuity sa handoff.
- Kapag pinaghihinalaang abuse, sundin agad ang mandated-reporting workflow at agency policy habang pinananatili ang patient safety.
- Para sa communication barriers, gumamit ng qualified interpreter pathways sa halip na ad hoc family translation para sa clinical decision-making discussions.
- Turuan ang pasyente/caregiver tungkol sa kahalagahan ng trend monitoring at follow-up expectations.
- Gumamit nang maingat ng skinfold-caliper findings dahil maaaring limitahan ng inter-operator variability ang consistency sa routine practice.
- Tapusin ang encounters sa safety sweep (call light, bed low/locked, reachable table, fall-hazard scan), pagkatapos ay magsagawa ng hand hygiene at equipment decontamination bago umalis.
Panganib sa Baseline Integrity
Ang hindi tumpak na initial measurements o malabong survey documentation ay maaaring magpaantala sa pagkilala ng tunay na clinical decline.
Parmakolohiya
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| diuretics | Furosemide, bumetanide | Maaaring mabilis baguhin ang weight at volume indicators; mahalaga ang trend interpretation. |
| corticosteroids | Prednisone-class agents | Maaaring baguhin ang weight distribution at fluid status sa paglipas ng panahon. |
Paglalapat ng Klinikal na Paghuhusga
Klinikal na Sitwasyon
Ang isang pasyente ay mukhang pagod na may shallow breathing at may hindi inaasahang pagtaas ng timbang kumpara sa baseline sa loob ng dalawang araw.
- Recognize Cues: Distress cues kasama ang abnormal anthropometric trend.
- Analyze Cues: Ang pinagsamang findings ay nagpapataas ng concern para sa umuusbong na fluid at cardiopulmonary stress.
- Prioritize Hypotheses: Agarang prayoridad ang pagkumpirma ng trend validity at pagsusuri ng physiologic impact.
- Generate Solutions: Ulitin ang measurement, kunin ang full vital signs, at magsagawa ng focused respiratory/cardiovascular assessment.
- Take Action: I-escalate ang validated concerns at ipatupad ang ordered monitoring/interventions.
- Evaluate Outcomes: Pinipigilan ng maagang aksiyon ang pag-usad sa severe decompensation.
Mga Kaugnay na Konsepto
- mga indicator ng vital signs ng physiologic functioning at homeostasis - Isinasama ang survey cues sa physiologic trend interpretation.
- pagsukat ng height para sa ambulatory residents - Technique standards para sa maaasahang height baselines.
- pagsukat ng timbang para sa ambulatory residents - Weight trend reliability para sa risk detection.
- pagpili ng uri ng nursing assessment - Pagpili ng comprehensive kumpara sa focused reassessment.
- pagdodokumento at pag-uulat ng data - Sinusuportahan ng objective charting ang ligtas na escalation at continuity.
Sariling Pagsusuri
- Aling general-survey cues ang dapat mag-trigger ng agarang focused reassessment?
- Bakit mahalaga ang standardized technique para sa anthropometric trend interpretation?
- Paano mababago ng maagang trend changes ang care priority bago lumitaw ang severe vital-sign abnormalities?