Stress at Anxiety
Mahahalagang Punto
- Ang stress ay tugon ng katawan-isipan sa perceived challenge; ang anxiety ay fear o unease na maaaring maging nakahahadlang kapag persistent.
- Maaaring adaptive ang acute stress, ngunit pinapalala ng chronic stress ang physical at psychiatric outcomes.
- Kabilang sa stress patterns ang acute, episodic acute, chronic, eustress, at distress na may magkaibang clinical implications.
- Ang unmanaged chronic stress ay maaaring magpahina ng needs sa physiologic stability, safety, belonging, esteem, at self-actualization.
- Sa nursing work, maaaring pahinain ng unmanaged distress ang team relationships, magpataas ng workplace errors, at magpabilis ng burnout/turnover.
- Umiiral ang anxiety sa continuum mula mild arousal hanggang panic-level dysregulation.
- Karaniwan ang anxiety burden: ang U.S. 12-month prevalence ay malapit sa one-fifth ng adults, na may mas mataas na reported prevalence sa females kaysa males.
- Pinagsasama ng nursing management ang coping-skills coaching, lifestyle supports, at targeted therapies.
- Sa life-limiting illness, madalas tumataas ang anxiety sa paligid ng prognosis, mortality, symptom burden, at perceived loss of control.
- Sa pediatric hospitalization, karaniwang co-regulates ang child anxiety sa caregiver emotional state at maaaring magpakita bilang separation distress, stranger distress, o temporary regression.
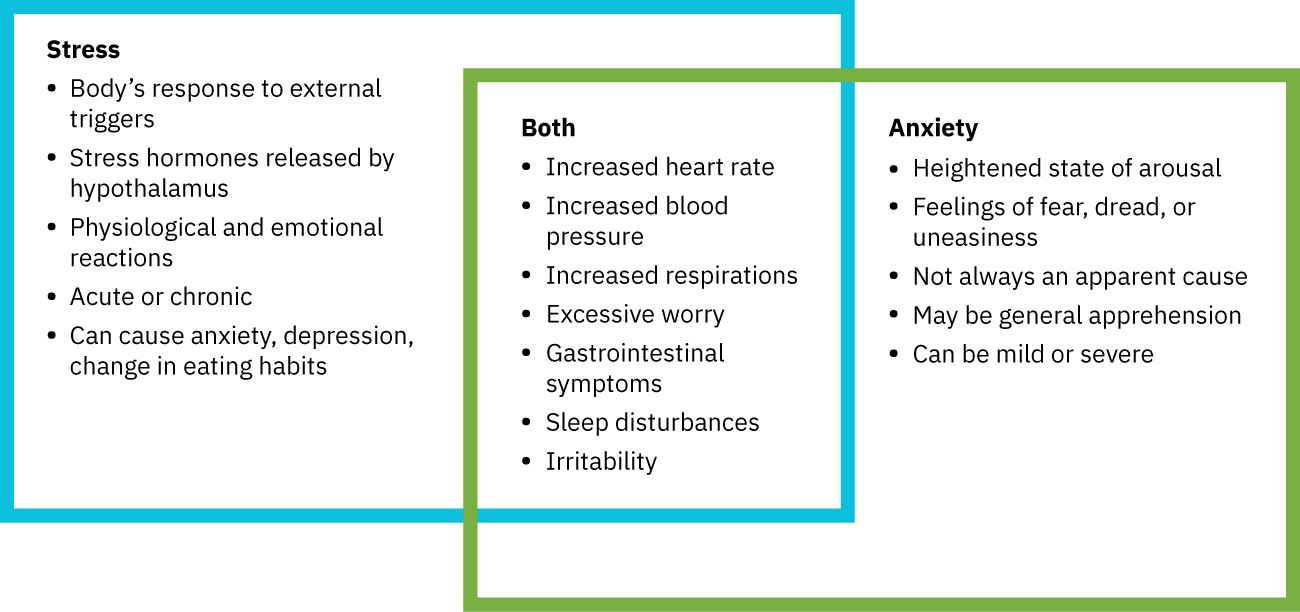 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.17.1.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.17.1.
Patopisyolohiya
Ina-activate ng stress ang sympathetic at neuroendocrine pathways (fight-or-flight), na nagpapataas ng heart rate, blood pressure, vigilance, at stress-hormone output. Isang core neuroendocrine sequence ang CRH release mula sa hypothalamus, ACTH release mula sa anterior pituitary, at cortisol release mula sa adrenal cortex, habang kasabay ang sympathetic catecholamine effects.
Karaniwang tugon ang fear sa immediate, identifiable threat, samantalang mas madalas na apprehension tungkol sa vague, anticipated, o uncertain threat ang anxiety; pareho nilang maaaring i-activate ang parehong physiologic stress-response systems.
Karaniwang time-limited ang acute stress at maaaring bumalik sa baseline kapag nakabawi. Ang paulit-ulit o matagal na activation na walang sapat na parasympathetic recovery ay maaaring magdisrupt ng sleep, immune function, metabolism, mood regulation, at cognition. Sa bedside teaching, karaniwang inilalarawan ang acute stress bilang short-term exposure, habang ang chronic stress ay persistent burden na tumatagal ng ilang buwan o higit pa.
Maaaring magpakita ang acute stress behavior bilang fight, flight, freeze, o fawn responses depende sa threat interpretation at prior experience.
Lumalabas ang anxiety disorders kapag nananatiling overactive at disproportionate sa actual threat ang fear-processing systems. Sa clinical setting, maaaring maging primary psychiatric disorder o secondary stress symptom sa panahon ng acute/chronic medical illness ang anxiety; maaari ring magpataas ng vulnerability ang family-history burden sa ilang patients.
Hinuhubog din ng appraisal ang response quality: maaaring maranasan ang parehong stressor bilang eustress (constructive activation) o distress (harmful burden) depende sa perception, coping resources, at contextual support. Mataas ang appraisal-dependence ng internal stressors at maaaring mag-iba ayon sa age, sex, prior experience, personal values, cultural o religious framework, at available resources, habang ang external stressors ay mula sa outside events (halimbawa infection, injury, o urinary retention).
Kapag nagpapatuloy ang chronic distress, maaaring magpatibayan sa isa’t isa ang physiologic strain at maladaptive behavior (halimbawa low energy na nagpapalala ng inactivity, poor diet, social withdrawal, o substance-related coping), na nagpapabilis ng long-term morbidity. Nag-iiba ang cognitive effects ayon sa stress phase: maaaring pansamantalang patalasin ng early alarm activation ang focus, habang madalas pinapahina ng prolonged stress ang information processing, rational decision-making, at memory reliability.
Binibigyang-diin ng psychophysiological stress model ang bidirectional cycling sa pagitan ng body at mind: maaaring magsimula ang anxiety bilang stress consequence, ngunit maaari rin itong maging bagong stressor na nagpapatuloy ng autonomic at endocrine activation.
Klasipikasyon
- Stress response domains: Physiologic, emotional, at behavioral reactions.
- Stress-duration domain: Acute stress (short-lived, recovery-capable) versus chronic stress (persistent activation at mas mataas na health burden).
- Stress subtype domains: Acute, episodic acute, chronic, eustress, at distress.
- Stress-valence domain: Neutral stress, positive adaptive stress (eustress), at negative harmful stress (distress).
- Stress-intensity continuum: Mula mild daily stress hanggang severe life-threatening stress exposure na may katumbas na escalation sa physiologic response.
- Stressor-origin domain: Physiologic stressors (illness, injury, pain, malnutrition, temperature extremes) at psychosocial stressors (grief, conflict, addiction, mental illness, ineffective coping).
- Stressor-location domain: Internal stressors (appraisal-driven interpretation) at external stressors (outside-body o environmental triggers).
- Stressor-scale domain: Significant life changes, catastrophic events, frequent annoyances, at omnipresent irritations.
- Common stressor domains: Environmental, lifestyle, major-life-event, organizational-routine, physiologic illness/pregnancy, at financial-pressure stressors.
- Stressor-context domain: Developmental stressors (lifespan milestones), situational stressors (unexpected personal events), at adventitious stressors (traumatic disaster/violence events).
- Life-stage vulnerability domain: Ang children (limited coping-language/regulation capacity) at older adults (cognitive/functional stress-amplifying factors) ay maaaring magpakita ng magkaiba ngunit clinically significant na stress responses.
- Appraisal domain: Stressor interpretation bilang growth challenge versus threat/harm expectation.
- Transactional model domain: Sumasalamin ang stress response sa person-environment transaction na hinuhubog ng personal, social, environmental, spiritual, cultural, educational, at emotional-regulation factors.
- Psychophysiological coupling domain: Mental distress na nagpapalakas ng physical strain at physical strain na nagpapalakas ng anxiety/distress.
- Coping domains: Problem-focused, emotion-focused, at resilience-oriented strategies.
- Coping quality: Adaptive (problem-solving, mindfulness, support use) versus maladaptive (avoidance, withdrawal, aggression, substance misuse).
- Defense-mechanism pattern: Maaaring maging adaptive sa limitadong paggamit ang protective responses, ngunit ang sobrang/maladaptive reliance ay maaaring magpalala ng functioning at psychiatric burden.
- Need-impact domain: Epekto sa physiologic function, safety/resource stability, belonging, esteem, at higher-level fulfillment.
- Self-regulation domains: Physiologic regulation (SNS-to-PNS balance), emotional regulation, at behavioral regulation na nakaayon sa long-term values.
- Anxiety-intensity levels: Mild, moderate, severe, at panic.
- Level progression cues: Mild (focused energy na may manageable restlessness), moderate (selective inattention, hampered learning/problem-solving, sympathetic activation), severe (markedly narrowed perceptual field, dazed/confused automatic behavior, at near-total loss of learning/problem-solving), panic (disorganized behavior at inability to process external cues).
- Panic-level profile: Maaaring kabilang ang pacing/running/shouting/screaming o abrupt withdrawal, occasional transient reality-contact disturbance, at post-episode exhaustion.
Nursing Assessment
Pokus sa NCLEX
Ihiwalay ang adaptive stress mula sa pathologic anxiety ayon sa duration, intensity, at functional impact.
- Suriin ang stressors, symptom pattern, at duration.
- Suriin ang stressor origin at scale upang linawin kung ang symptoms ay pangunahing physiologic-triggered, psychosocial-triggered, o halo.
- Suriin ang individualized stress response drivers, kabilang ang physical state, emotional state, at cognitive understanding/appraisal ng stressor.
- Suriin ang appraisal modifiers na nagpapabago sa internal stressor intensity, kabilang ang age, sex, lived experience, values, cultural/religious beliefs, at practical resources.
- Suriin ang transactional context (social supports, environment, spirituality/culture, educational background, at emotional-regulation capacity) dahil binabago nito ang stress-response trajectory.
- Ihiwalay ang stress subtype (acute, episodic acute, chronic, eustress, o distress) at functional impact nito.
- Suriin ang personal adaptation factors: baseline coping capacity, current health burden, support-system reliability, at SES/SDOH constraints.
- Suriin ang predisposing risk factors para sa poor adaptation, kabilang ang early-life adversity (halimbawa prenatal stress at ACE burden), chronic optimism/pessimism pattern, previous coping failures, at unresolved health/surgical sequelae.
- Direktang suriin ang life-stage modifiers: maaaring limitado ang stress vocabulary at impulse-control coping ng children, habang maaaring may cognitive slowing, mobility decline, at independence-related stress amplification ang older adults.
- Suriin kung aling need levels ang disrupted (physiologic, safety/resources, belonging, esteem, at self-actualization goals).
- Suriin ang acute autonomic cues (elevated heart rate/respiratory rate/blood pressure, dilated pupils, diaphoresis).
- Sa moderate anxiety, suriin ang selective inattention kasama ng physiologic cues tulad ng sweating, tachycardia/tachypnea, headache, gastric discomfort, urinary urgency, voice tremor, at shakiness.
- Sa severe anxiety, suriin ang hyperventilation, pounding heart, insomnia, confusion/dazed presentation, automatic behavior, at expressed sense of impending doom.
- Suriin ang distress-linked emotional at somatic cues (halimbawa unease, sadness, pain, at nonspecific symptom clusters na mahirap i-localize).
- Suriin ang chronic stress patterns (irritability, fatigue, headache, poor concentration, insomnia, digestive changes, appetite changes, helplessness, low self-esteem, frequent illness, reduced sexual desire).
- Suriin ang overlap pattern ng acute-on-chronic burden (halimbawa bagong injury/infection na nakapatong sa chronic illness) dahil maaaring mabilis mapalala ng combined stressors ang coping at physiologic stability.
- Suriin ang cumulative stress stacking (multiple simultaneous stressors) at practical burden barriers (cost, transportation, income loss, at care-access friction).
- Suriin ang withdrawal-associated stress physiology sa at-risk patients (halimbawa anxiety na may tachycardia at marked hypertension pagkatapos ng abrupt substance cessation).
- Kapag persistent ang anxiety, i-trend ang severity gamit ang structured self-report tools kung available (halimbawa STAI at BAI) at iugnay sa functional impairment.
- Gumamit ng objective adjuncts kung kailangan (halimbawa heart rate/blood pressure/respiratory trends, ECG-based autonomic response, o skin-conductance measures) habang kinikilalang clinical at subjective diagnosis pa rin pangunahing batayan ng anxiety.
- Kung hindi malinaw ang presentation at context, isama ang behavior-based assessment (halimbawa approach-avoidance response sa feared stimuli) na may safety safeguards.
- Suriin ang multidomain distress manifestations sa workforce settings: physical (halimbawa headache, sleep disruption, palpitations/blood-pressure elevation, GI changes, tremor, diaphoresis), mental (halimbawa anger, irritability, mood change, isolation, reduced confidence), at behavioral (halimbawa increased alcohol/substance use, appetite shift, conflict escalation, workplace error increase).
- Suriin ang cognitive distortions (catastrophizing, all-or-nothing thinking, overgeneralization, jumping to conclusions, personalization, at threat overestimation).
- Suriin ang kasalukuyang pagiging epektibo ng coping style at available social supports.
- Suriin ang support-system strength dahil pinapataas ng mahinang family/friend support ang risk ng persistent distress.
- Suriin ang safety concerns, kabilang ang escalation sa panic, self-harm risk, o substance misuse.
- Suriin kung physiologically stress-induced ang anxiety dahil sa active medical illness (halimbawa severe cardiopulmonary o pain crises) bago magtapos sa primary anxiety disorder conclusion.
- Suriin ang colleague-observed stress signals (halimbawa irritability, withdrawal, fatigue, error increase, o absenteeism) dahil maaaring mas maagang matukoy ng external observation ang distress kaysa self-report.
- Sa pediatric-family contexts, suriin ang dyadic escalation patterns (caregiver anxiety transmission, prolonged goodbye patterns, at child loss-of-control behavior sa ilalim ng hospitalization stress).
- Mag-screen para sa panic features (palpitations, chest discomfort, paresthesias, lightheadedness, depersonalization, acute fear of losing control) at ituring na urgent ang sudden severe presentations habang inaalis ang medical emergencies.
- Ihiwalay ang panic bilang continuum-level anxiety state mula sa DSM-defined panic-attack episode na may specific diagnostic criteria.
- Suriin ang stress-related cognitive performance (processing speed, concentration, memory recall, at decision quality), lalo na sa high-stakes care discussions.
Nursing Interventions
- Ituro ang grounding, paced breathing, at relaxation techniques para sa acute symptom reduction.
- Palakasin ang adaptive self-regulation practices gaya ng reflection/journaling, healthy boundary setting, structured positive self-talk, at psychotherapy referral kapag nagpapatuloy ang maladaptive defense patterns.
- Kapag prominent ang defense mechanisms, gumamit ng nonjudgmental active listening at open-ended exploration sa halip na direct confrontation, pagkatapos suportahan ang unti-unting insight habang handa ang pasyente.
- Ituro ang relaxation breathing: komportableng posisyon, mabagal na diaphragmatic breaths, inhale/exhale counts, at minimum 5-minute practice.
- I-coach ang problem-solving at time-management skills para sa controllable stressors.
- Gumamit ng stepwise adaptation coaching: tukuyin ang predisposing risk factors, tukuyin ang stressor, linawin ang personal feelings, pumili ng prioritized actions, at muling suriin ang outcomes.
- Para sa physiologic stressors, unahin ang cause-directed care (halimbawa hydration, pain control, nutrition support, temperature management) habang mino-monitor ang pagbabalik sa baseline.
- Para sa external physiologic stressors (halimbawa infection/injury o urinary retention), unahin ang direct trigger relief (gaya ng antimicrobials, procedures, o catheterization kapag indicated) upang mabawasan ang ongoing stress activation.
- Kapag ang medical illness ang malamang stressor, gamutin ang underlying physiologic trigger habang sabay na gumagamit ng anxiety-reduction communication at coping support.
- Itaguyod ang sleep hygiene, activity, at nutrition upang mabawasan ang physiologic burden.
- Para sa chronic distress cycles, ipares ang symptom care sa health-habit reset plans (nutrition, activity, tobacco/substance reduction, at social reconnection).
- Bumuo ng practical daily coping plans: magtakda ng boundaries, gumamit ng realistic expectations, iwasan ang alcohol/illicit drugs/tobacco coping, at mag-iskedyul ng social connection.
- Magkasamang magdisenyo ng constructive actions na nagpapabuti sa access sa coping resources (halimbawa mobility aid placement, water availability, at practical support setup) at iwasan ang destructive options na nagdadagdag ng secondary distress.
- Ihiwalay ang willingness mula sa ability to change at gumamit ng motivational interviewing kasama ng staged goals kapag halo ang readiness.
- I-coach ang diet-related stress hygiene sa pamamagitan ng paglimita sa simple carbohydrates, excess caffeine, at stress-related overeating patterns.
- Ituro ang WHO-style micro-skills para sa intrusive stress reactions: grounding, unhooking, values-based action, kindness, at paggawa ng espasyo para sa mahihirap na damdamin.
- Ituro ang practical grounding sequence para sa acute overload: pansinin ang thoughts/feelings, bagalan ang paghinga, muling kumonekta sa body posture, at mag-orient gamit ang five-senses prompts.
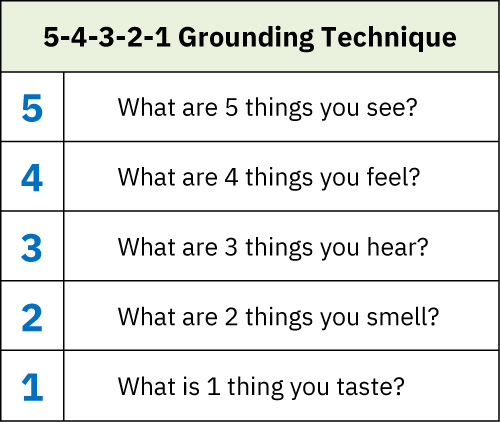 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.17.1.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.17.1. - Gumamit ng brief reality reorientation kasama ng paced breathing kapag hindi proporsyonal sa objective danger ang perceived threat, upang mabawasan ang sympathetic escalation.
- Gumamit ng compassionate pacing at active listening upang matukoy ang highest-priority concern ng patient, na maaaring iba sa inaakalang stressors.
- Magbigay ng malinaw na written information at ulitin ang key teaching kapag mataas ang stress burden dahil maaaring mabawasan ang real-time cognitive processing.
- Ituro ang unhooking sequence para sa intrusive thoughts: notice, name (“I notice…”), at refocus sa present task o tao.
- Gumamit ng brief cognitive reframing prompts (halimbawa, “What is the worst realistic outcome right now?”) upang putulin ang catastrophic thought spirals.
- Ituro ang mindfulness sa nonjudgmental present-centered terms: pansinin ang thoughts/feelings habang lumilitaw, tanggapin ang presensya ng mga ito, at pumili ng deliberate response sa halip na automatic reaction.
- Ituro ang world-events stress hygiene: limitahan ang paulit-ulit na news/social-feed exposure, magsagawa ng maikling self-check bago magbasa ng mabibigat na headlines, at mag-iskedyul ng screen-disconnection periods.
- Mag-alok ng emotion-focused options gaya ng mindfulness meditation, guided imagery, at yoga kapag nakaayon sa client preference at capacity.
- Para sa selected clients na may access sa trained-provider, isaalang-alang ang adjunctive biofeedback o hypnotherapy bilang bahagi ng mas malawak na anxiety-management plan.
- Isama ang humor-based reframing at safe laughter activities bilang optional emotion-focused coping tools kapag culturally appropriate at katanggap-tanggap sa client.
- Sanayin ang self-regulation skills sa pamamagitan ng pagpares ng symptom awareness (breath, heart rate, muscle tension) sa intentional PNS-activating techniques.
- Hikayatin ang routine self-monitoring gamit ang brief standardized stress tools (halimbawa perceived-stress screening) upang maagang matukoy ang distress escalation.
- Palakasin ang resilience-building habits at support-network engagement.
- Palakasin ang resilience sa prolonged public stress periods: panatilihin ang preventive health routines, protektahan ang sleep/activity/nutrition basics, at gumamit ng intentional phone/video social connection upang mabawasan ang isolation.
- Gumamit ng peer-support communication kapag napapansin ang harmful stress signs (halimbawa nonjudgmental “I noticed…” check-ins) at maagang ibahagi ang formal support options.
- I-coordinate ang psychotherapy/pharmacotherapy referral kapag nakahahadlang sa function ang anxiety.
- Gumamit ng physical down-regulation techniques gaya ng breathing-based biofeedback at short cooling-compress application sa head/face/neck kapag clinically appropriate.
- I-optimize ang healing environment cues sa pamamagitan ng pagbawas ng noise/news exposure (halimbawa pagpatay sa distressing media at paggamit ng calming/nature audio kapag available).
- Para sa extreme anxiety o panic, manatili kasama ng client, bawasan ang environmental stimuli, gumamit ng calm/brief reassurance, at unahin ang immediate safety.
- Sa pediatric separation distress, i-coach ang caregivers na gumamit ng calm brief goodbyes, panatilihin ang predictable routines, at gumamit ng familiar comfort objects/distraction sa halip na prolonged reassurance cycles na nagpapataas ng anxiety.
- Talakayin ang complementary approaches (halimbawa massage, acupuncture, chamomile, kava, melatonin, lavender) nang may pag-iingat dahil halo ang ebidensya at maaaring may interaction risk.
Chronic-Stress Normalization
Ang pagtrato sa severe chronic stress bilang “normal life pressure” ay nagpapaliban ng care at nagpapataas ng morbidity.
Pharmacology
Maaaring kabilang sa medication options para sa anxiety ang SSRIs/SNRIs, buspirone, at short-term benzodiazepine use sa selected contexts. Dapat subaybayan ng nursing care ang dependency risk, withdrawal risk, side effects, at functional response.
Aplikasyon ng Clinical Judgment
Klinikal na Sitwasyon
Isang client ang nag-uulat ng persistent worry, insomnia, muscle tension, gastrointestinal upset, at humihinang concentration sa trabaho sa loob ng ilang buwan.
- Recognize Cues: Multi-domain anxiety burden na may functional decline.
- Analyze Cues: Lumalampas ang pattern sa short-term adaptive stress response.
- Prioritize Hypotheses: Prayoridad ang anxiety disorder evaluation at immediate coping support.
- Generate Solutions: Pagsamahin ang symptom-regulation skills at therapy/medication pathway.
- Take Action: Ipatupad ang grounding education, sleep plan, at referral coordination.
- Evaluate Outcomes: Muling suriin ang anxiety severity, function, at coping capacity.
Mga Kaugnay na Konsepto
- mga anxiety-related disorder - Pinapalawak ang diagnosis-specific anxiety conditions at interventions.
- sariling pananakit at pagpapakamatay - Tinutugunan ang escalation risk sa severe anxiety/depressive overlap.
- spectrum ng mood disorders - Sumusuporta sa differential evaluation kasama ng mood-spectrum states.
- mga trauma-induced at stress-related disorder - Iniuugnay ang chronic stress responses sa trauma syndromes.
- pakikilahok ng client - Pinapabuti ang adherence sa anxiety-management plans.