Regulasyon ng Fluid at Electrolyte Ayon sa mga Organo
Mahahalagang Punto
- Ang total body fluid ay pangunahing nire-regulate ng renal system.
- Ang kidneys ay paulit-ulit na umiikot ng humigit-kumulang 5 to 6 liters ng dugo at gumagawa ng about 200 liters ng daily filtrate bago ang selective reabsorption.
- Kapag mababa ang body fluid (hypovolemia), tumataas ang antidiuretic hormone (ADH) release na nagpapataas ng renal water reabsorption.
- Kapag mataas ang renal tubular fluid volume, nasu-suppress ang ADH, na nag-aambag sa mas dilute na urine.
- Ang serum osmolality ay normal na about 275-295 mmol/kg at sumasalamin sa blood concentration status.
- Ang osmolality ay solute particles per kilogram of solvent, habang ang osmolarity ay solute particles per liter of solvent.
- Ang urine specific gravity ay normal na about 1.010-1.020; ang mas mataas na values ay nagmumungkahi ng concentration at ang mas mababa ay nagmumungkahi ng dilution.
- Ang thirst, hypothalamic osmoreceptors, ADH, at RAAS ay nagko-coordinate ng intravascular volume at blood pressure.
- Ang RAAS ay maaaring ma-activate ng hypotension o low serum sodium at nagpapataas ng vascular tone plus sodium-water retention habang itinataguyod ang potassium excretion.
- Ang aldosterone ay key regulator ng sodium at potassium handling sa renal physiology at sumusuporta sa water retention sa pamamagitan ng sodium reabsorption.
- Sa stable adults, ang daily fluid output ay mostly renal (about 60%) at ang natitira ay insensible skin/GI/lung losses (about 40%).
- Ang cardiac natriuretic peptides ay kumokontra sa RAAS sa panahon ng fluid overload sa pamamagitan ng pag-promote ng vasodilation at sodium-water excretion.
- Ang homeostatic control ay gumagamit ng receptor → control center → effector signaling loops para iwasto ang deviation mula sa set points.
- Ang negative feedback ang pangunahing homeostatic loop pattern at kumikilos sa pamamagitan ng pagbaliktad sa deviation mula sa normal range.
- Ang positive feedback ay nagpapalakas ng stimulus para sa mabilis na pagkumpleto ng specific biologic events at dapat agad tumigil para maiwasan ang instability.
- Parehong ang hyperosmolality at hypoosmolality ay maaaring magdulot ng severe neurologic deterioration kapag hindi naitama agad.
- Ang failure sa sensing, loop activation, response execution, o set-point regulation ay maaaring lumala tungo sa cellular injury at organ dysfunction.
- Ang electrolyte abnormalities ay madalas na interdependent, kaya ang isang severe disturbance ay maaaring mag-trigger ng multi-electrolyte chain reaction.
Patopisyolohiya
Ang fluid at electrolyte homeostasis ay nakadepende sa interaction sa pagitan ng organ systems at hormones kaysa sa isolated laboratory values. Nire-regulate ng kidneys ang total body fluid at tumutugon sa tubular pressure at volume conditions sa pamamagitan ng ADH modulation. Ang kidney filtration ay pressure dependent: ang hydrostatic forces sa glomerular capillaries ay sumusuporta sa filtrate formation, at ang mababang renal perfusion pressure ay maaaring magpababa ng waste at fluid clearance.
Kapag may fluid loss at tumataas ang intravascular sodium concentration, tumataas ang serum osmolality. Ang hypothalamic osmoreceptors ay nagti-trigger ng thirst at nagpapataas ng ADH release, na nagpo-promote ng renal water retention. Ang regulatory pathway na ito ay nakadepende sa functional access sa fluids at kakayahang uminom kapag may thirst cues.
Sinusuportahan din ng RAAS ang perfusion sa low-pressure states at low-sodium states. Ang nabawasang blood pressure o nabawasang serum sodium ay nagpapasigla ng renal renin release. Kino-convert ng renin ang liver-derived angiotensinogen sa angiotensin I, at kino-convert ng angiotensin-converting enzyme sa baga ang angiotensin I sa angiotensin II. Ang angiotensin II ay nagdudulot ng vasoconstriction at nagpapasigla ng aldosterone release, na nagpapataas ng renal sodium reabsorption kaya sumusunod ang tubig papasok sa intravascular compartment habang tumataas ang potassium excretion.
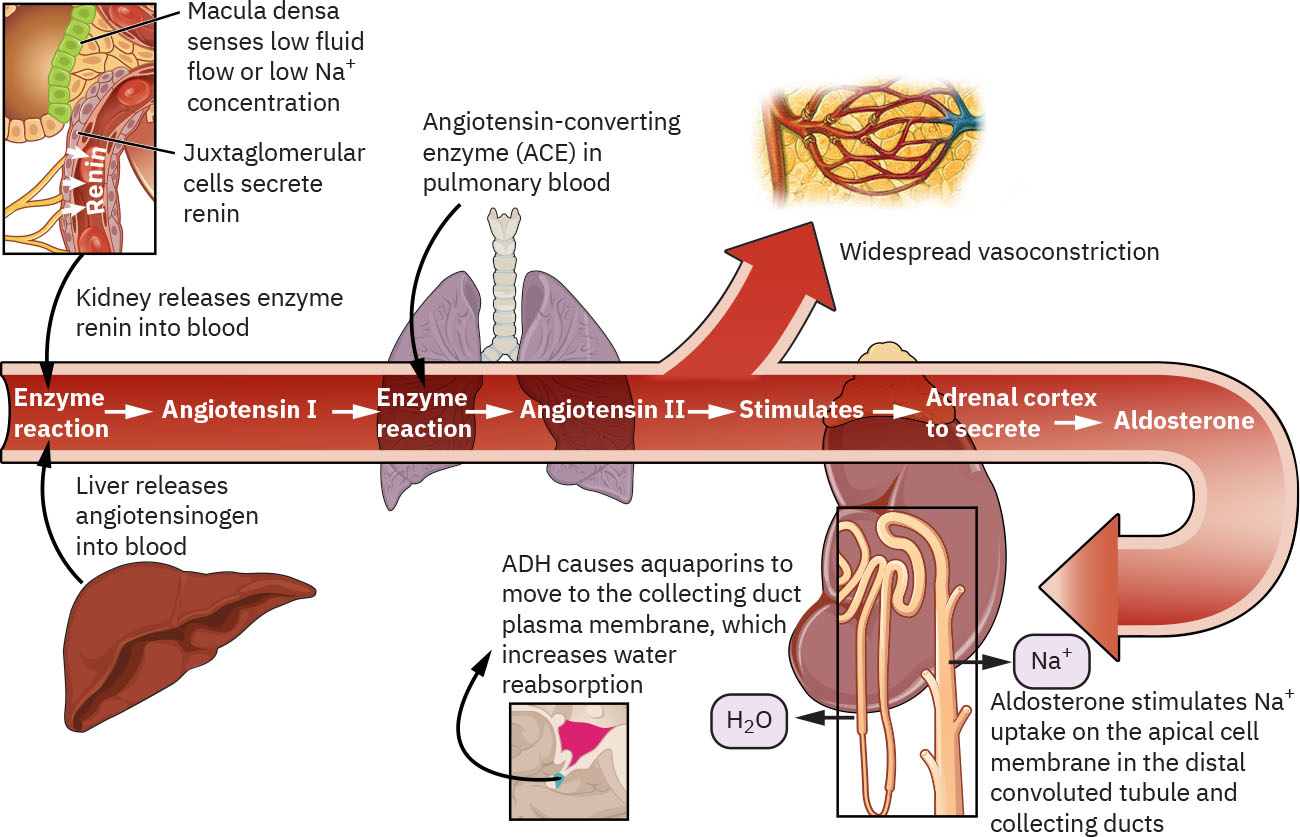 Illustration reference: OpenStax Clinical Nursing Skills Ch.19.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.19.1.
Ang natriuretic peptides ay kumikilos bilang physiologic opposition sa RAAS. Kapag nararamdaman ng cardiac tissue ang fluid overload at elevated pressure, ang mga peptide na ito ay nagpo-promote ng vasodilation at renal sodium excretion para mabawasan ang circulating volume at pressure. Kasama ng ADH, RAAS, at natriuretic peptides, ang endocrine factors gaya ng insulin, epinephrine, glucocorticoids, at parathyroid-axis hormones ay nakaaapekto sa specific electrolyte patterns. Ang renin release ay nire-regulate din sa bahagi ng juxtaglomerular apparatus malapit sa glomerulus, na direktang nag-uugnay ng nephron perfusion sensing sa RAAS activation.
Kung sapat ang intake, ang kidneys ay karaniwang gumagawa ng around 1,500 mL ng urine araw-araw. Ang oliguria ay early warning sign sa fluid-deficit at kidney-injury pathways at dapat i-trend kasama ng konteksto.
Pag-uuri
- Volume-conserving response: Increased ADH sa hypovolemia na may increased water reabsorption.
- Volume-excreting response: ADH suppression kapag mataas ang tubular fluid volume, na nagreresulta sa dilute urine.
- Osmoreceptor-thirst response: Ang increased serum osmolality ay nagtutulak ng thirst at ADH release.
- Osmolality measurement domain: Tinutukoy ng osmolality ang particles per kg solvent; tinutukoy ng osmolarity ang particles per L solvent.
- Hyperosmolality pattern: High-solute state (halimbawa dehydration o diabetes-linked states) na may risk para sa circulatory stress at neurologic symptoms.
- Hypoosmolality pattern: Low-solute state (halimbawa excess free water o water-balance dysregulation) na may risk para sa cerebral edema at neurologic decline.
- RAAS pressure-restoring response: Renin → angiotensin II → aldosterone ay nagpapataas ng vascular tone at sodium-water retention.
- RAAS sequence detail: Renin + angiotensinogen (liver) → angiotensin I → ACE (lungs) → angiotensin II.
- Natriuretic-peptide counterregulation: Ang cardiac peptides ay tumutugon sa fluid overload/high pressure sa pamamagitan ng pag-promote ng vasodilation at sodium-water excretion.
- Feedback-loop control architecture: Ang receptor detection, central integration, at effector response ay nagko-coordinate ng correction ng fluid/electrolyte deviation.
- Negative-feedback loop pattern: Ang inhibitory response ay nagpapababa ng initial deviation at ibinabalik ang variables patungo sa set point.
- Positive-feedback loop pattern: Ang amplifying response ay nagpapataas ng initial stimulus hanggang endpoint completion (halimbawa clot formation, lactation let-down, at uterine contraction sa panganganak).
- Homeostatic-failure modes: Detection failure, feedback-initiation failure, effector-response failure, at set-point dysregulation.
- Sodium regulation pathway: Renal system na may aldosterone influence.
- Potassium regulation pathway: Renal system na may aldosterone plus insulin, epinephrine, at glucocorticoids.
- Calcium regulation pathway: Skeletal-endocrine interaction na may parathyroid hormone, vitamin D, at calcitonin.
Pagtatasa sa Nursing
Pokus sa NCLEX
Itugma muna ang symptoms sa malamang na regulated electrolyte pathway, pagkatapos ay i-verify gamit ang labs at volume trend.
- I-track ang intake at output, urine concentration pattern, at net fluid balance para sa ADH-related volume cues.
- I-trend ang serum osmolality kasama ng urine osmolality/specific-gravity patterns kapag hindi malinaw ang dilution versus concentration status.
- Suriin kung ang functional barriers (cognitive change, weakness, poor access to fluids) ay naglilimita sa pagtugon sa thirst cues.
- Suriin ang low-perfusion compensatory patterns (halimbawa tachycardia na may hypotension) na maaaring mauna sa lumalalang renal filtration.
- Para sa sodium imbalance, suriin ang confusion, irritability, thirst, dry mucous membranes, headache, seizure risk, at coma progression.
- Para sa potassium imbalance, suriin ang GI cramping, weakness, pulse quality, at ECG changes kabilang ang peaked o flattened/inverted T waves at U-wave patterns.
- Para sa calcium imbalance, suriin ang GI symptoms, muscle weakness, tingling, cramps, at tetany.
- I-escalate ang low urine output trends, kabilang ang persistent output below 30 mL/hour (o below 0.5 mL/kg/hour) over 8 hours.
- I-correlate ang symptom patterns sa serial chemistry values at clinical trajectory.
- Kapag lumalala ang fluid retention pero bumababa ang urine output, isaalang-alang ang mixed patterns kung saan mas diluted ang serum habang nananatiling relatively concentrated ang urine.
Mga Interbensyon sa Nursing
- I-prioritize ang maagang intervention kapag ang volume o neurologic trends ay nagmumungkahi ng failure ng compensatory regulation.
- I-coordinate ang serial labs at focused reassessment para matukoy kung naibabalik ng organ-level regulation ang balance.
- Ipatupad ang ordered fluid strategies at i-monitor ang urine response para sa inaasahang ADH-linked effects.
- I-monitor ang daily intake/output patterns laban sa inaasahang adult water-balance ranges (approximately 2,500 mL intake at 2,500 mL output sa stable conditions).
- Palakasin ang sodium at potassium management education sa mga pasyenteng may chronic renal at endocrine risk factors.
- I-escalate agad kapag ang ECG o neurologic findings ay nagpapahiwatig ng severe electrolyte instability.
Compensation Limits
Ang organ-hormone compensation ay protective sa acute states ngunit hindi nito lubusang napipigilan ang deterioration sa chronic disease o severe imbalance.
Farmakolohiya
| Klase ng Gamot | Mga Halimbawa | Mahahalagang Pagsasaalang-alang sa Nursing |
|---|---|---|
| diuretics(mga diuretic) | Loop at potassium-sparing na mga kategorya | Binabago ng diuretics ang sodium, potassium, at fluid balance at nangangailangan ng close trend monitoring. |
| intravenous-fluid-categories-tonicity-and-infusion-regulation(electrolyte-replacement therapy) | Mga protocol para sa sodium o potassium replacement | Ang correction ay dapat gabayan ng serial labs, renal status, at symptom severity. |
Aplikasyon ng Clinical Judgment
Klinikal na Sitwasyon
Ang pasyenteng may chronic kidney disease ay nagkakaroon ng fluid retention, electrolyte abnormalities, at evolving neurologic symptoms.
- Recognize Cues: Abnormal fluid balance, urine pattern change, at concerning sodium/potassium symptom profile.
- Analyze Cues: Nabibigo ang renal-endocrine regulation na mapanatili ang homeostasis.
- Prioritize Hypotheses: Ang agarang risks ay neurologic decline at cardiac conduction instability.
- Generate Solutions: Paigtingin ang monitoring, kumuha ng serial labs/ECG, at ilapat ang ordered volume-electrolyte correction.
- Take Action: I-escalate ang deterioration at ipatupad ang cause-directed management.
- Evaluate Outcomes: Nagte-trend patungo sa stable baseline ang urine, labs, at symptoms.
Kaugnay na Konsepto
- mga karamdaman sa balanse ng sodium - Ang sodium findings ay tumutugma sa renal-aldosterone regulation failure o overload states.
- mga karamdaman sa balanse ng potassium - Ang potassium instability ay sumasalamin sa renal handling at hormone-modulated shifts.
- fluid volume deficit, hypovolemia, at dehydration - Ang low volume state ay nagtutulak ng ADH-mediated water conservation.
- fluid volume overload at hypervolemia - Ang high-volume states ay maaaring kasabay ng suppressed ADH at dilutional patterns.
- sakit sa bato - Ang chronic renal dysfunction ay nagpapababa ng kapasidad para mapanatili ang fluid-electrolyte homeostasis.
Sariling Pagsusuri
- Paano naiiba ang ADH behavior sa hypovolemia kumpara sa high tubular fluid volume states?
- Aling symptom clusters ang nagmumungkahi ng sodium versus potassium versus calcium dysregulation?
- Bakit maaaring pumalya ang compensation sa mga pasyenteng may chronic renal disease kahit activated ang hormonal pathways?