Peripheral Vascular System at Mga Pattern ng Insufficiency
Mahahalagang Punto
- Kabilang sa peripheral vascular system ang arteries, veins, arterioles, venules, at capillary networks na nagpapanatili ng tissue perfusion.
- Sinusuportahan ng peripheral vascular system ang whole-body homeostasis sa pamamagitan ng pamamahagi ng oxygen/nutrients at pag-aalis ng metabolic waste.
- Ang arteriosclerosis ay tumutukoy sa pagkapal at pagtigas ng arterial wall, samantalang ang atherosclerosis ay tumutukoy sa inflammatory plaque buildup (madalas na mayaman sa LDL) sa loob ng arterial walls.
- Ang arterial insufficiency at venous insufficiency ay may magkakaibang pattern ng pain, skin, pulse, at edema.
- Ang intermittent claudication ay mahalagang cue para sa peripheral arterial disease (PAD) at dapat mag-trigger ng focused vascular follow-up.
- Sinusuri ang acute limb perfusion decline gamit ang 6 P findings: pain, paralysis, paresthesia, pulselessness, pallor, at poikilothermia.
- Ang PAD na may persistent ischemia ay maaaring umusad sa nonhealing wounds, amputation risk, at mas mataas na panganib ng myocardial infarction at stroke.
- Ang chronic venous insufficiency ay sumasalamin sa hindi epektibong lower-extremity venous return na may dependent pooling na karaniwang lumalala habang tumatagal ang araw.
- Mas mataas ang venous-insufficiency burden sa older adults, mga taong may obesity, at mga babae.
- Mataas ang PAD burden sa buong mundo at tumataas ito sa mas matandang edad, smoking exposure, diabetes, at kasabay na cardiovascular disease.
Patopisyolohiya
Namamahagi ang peripheral vessels ng oxygen, nutrients, hormones, at heat-regulation capacity sa mga tissue habang ibinabalik ang deoxygenated blood at metabolic waste sa central circulation. Nakasalalay ang flow dynamics sa vessel tone, valve function, at pressure gradients.
Sumusunod ang systemic flow sa organisadong vascular path: aorta → arteries → arterioles → capillaries → venules → veins. Ang pagkakasunod na ito ang balangkas sa bedside interpretation kung saan pinaka-malamang nagaganap ang perfusion loss o venous return failure.
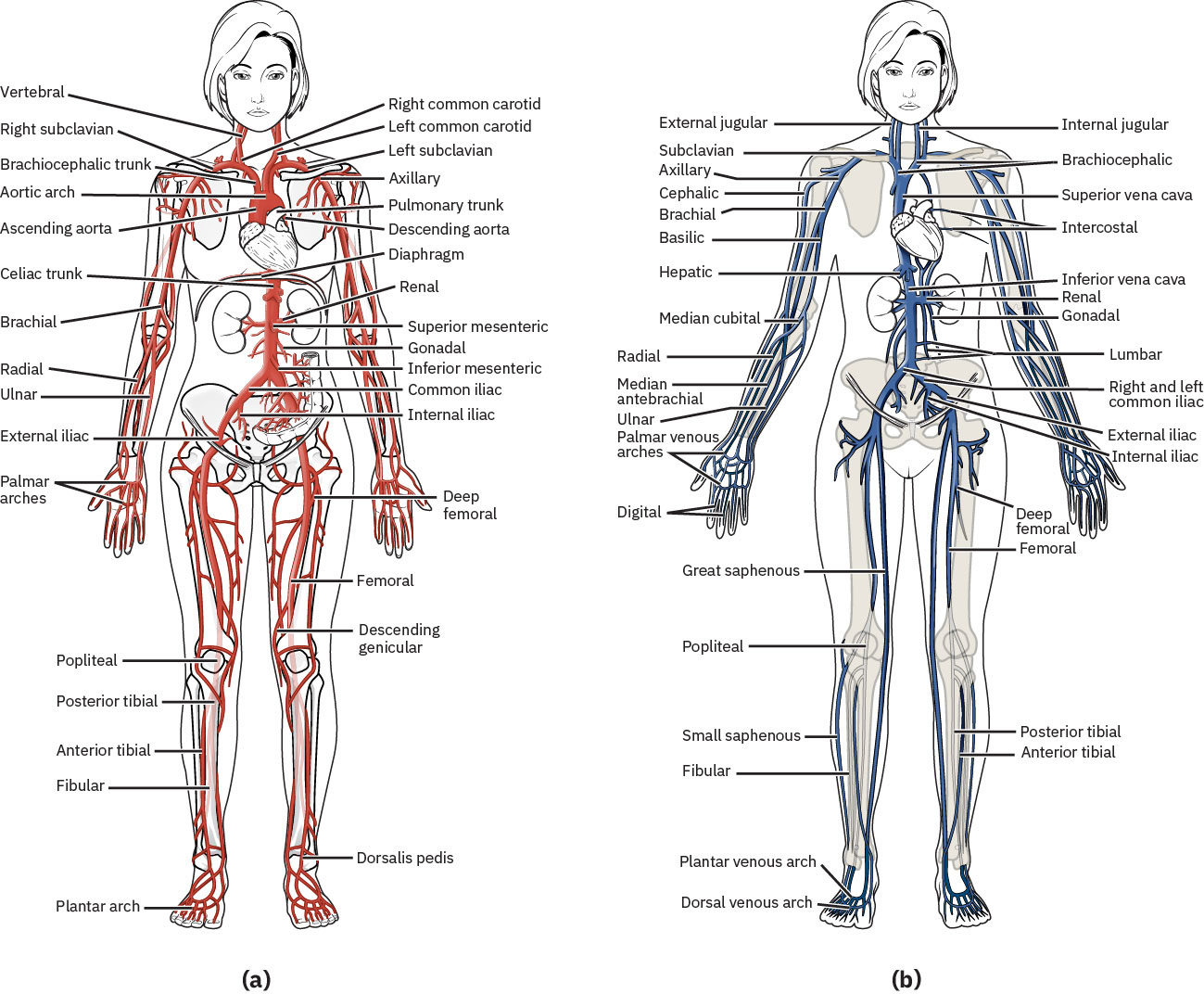 Illustration reference: OpenStax Clinical Nursing Skills Ch.24.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.24.2.
Ang peripheral arterial disease (PAD) ay kadalasang nakaaapekto sa lower-extremity arteries, kung saan ang progressive atherosclerotic narrowing ay nagpapababa ng paghahatid ng oxygenated blood sa oras ng exertion at maaaring umusad sa ischemic tissue injury. Ang carotid-artery stenosis ay high-yield na occlusive vascular pattern dahil tumataas ang stroke probability sa cerebral hypoperfusion at embolic risk; ang clinically significant carotid narrowing ay marker din ng mas malawak na systemic arterial disease. Parehong naaapektuhan ang mga lalaki at babae na lampas 60 taong gulang ng PAD, at ang kasabay na CAD, aortic disease, o carotid disease ay dapat magpataas ng hinala sa peripheral-arterial involvement.
Ang occlusive processes (gaya ng plaque o thrombus) at functional dysregulation (abnormal vasoconstriction o vasodilation) ay parehong maaaring magpababa ng epektibong perfusion at magdulot ng ischemic injury. Madalas na magkasabay ang arteriosclerosis at atherosclerosis; ang arterial stiffening ay nagpapababa ng vascular adaptability, at ang plaque progression ay lalo pang nagpapakipot ng lumen diameter at nagpapalala ng daloy. Kapag natukoy ang carotid disease, dapat isaalang-alang ang kasabay na aortic at renal-artery disease burden sa risk stratification at follow-up planning.
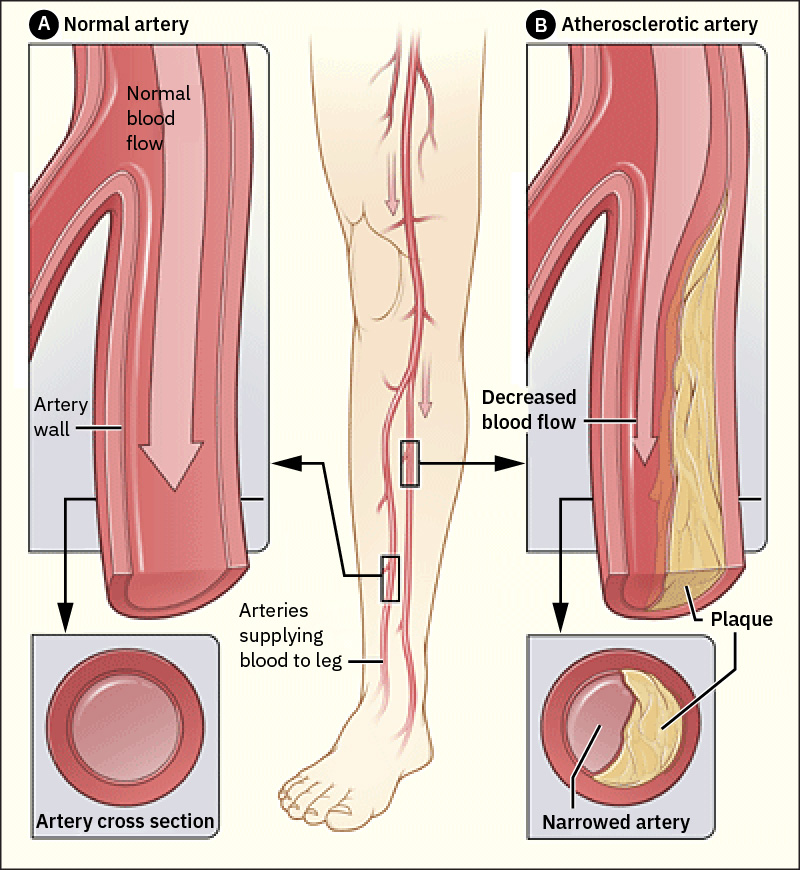 Illustration reference: OpenStax Clinical Nursing Skills Ch.24.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.24.2.
Nakaaapekto rin ang peripheral vascular dysfunction sa iba pang care domains, kabilang ang wound-healing trajectory, perioperative risk, at chronic disease management plans.
Ang arteries ay smooth-muscle, elastic vessels na lumalawak sa systole at bumabalik sa dating hugis sa diastole; ang pressure-wave transmission na ito ang nakakapkap bilang peripheral pulse. Sinusuportahan din ng arteries ang nutrient/hormone delivery at thermoregulation bukod sa oxygen transport.
Ang arterioles ay pangunahing resistance site at mahigpit na kinokontrol ng sympathetic signaling at vasoactive mediators. Binabago ng catecholamine effects at circulating/local mediators (halimbawa angiotensin II at prostaglandins) ang arteriolar diameter at samakatuwid ang distribusyon ng tissue perfusion.
Ang veins ay thin-walled, low-pressure, high-capacitance vessels na umaasa sa skeletal-muscle contraction at respiratory pressure changes upang ilipat ang dugo patungo sa puso. Tumutulong ang intraluminal venous valves upang mapanatili ang one-way forward flow at limitahan ang backward pooling. Kapag humina ang valve competence, maaaring magdulot ang venous reflux ng retrograde pooling sa lower-extremity circulation at pabilisin ang pag-usad ng chronic venous-insufficiency symptoms.
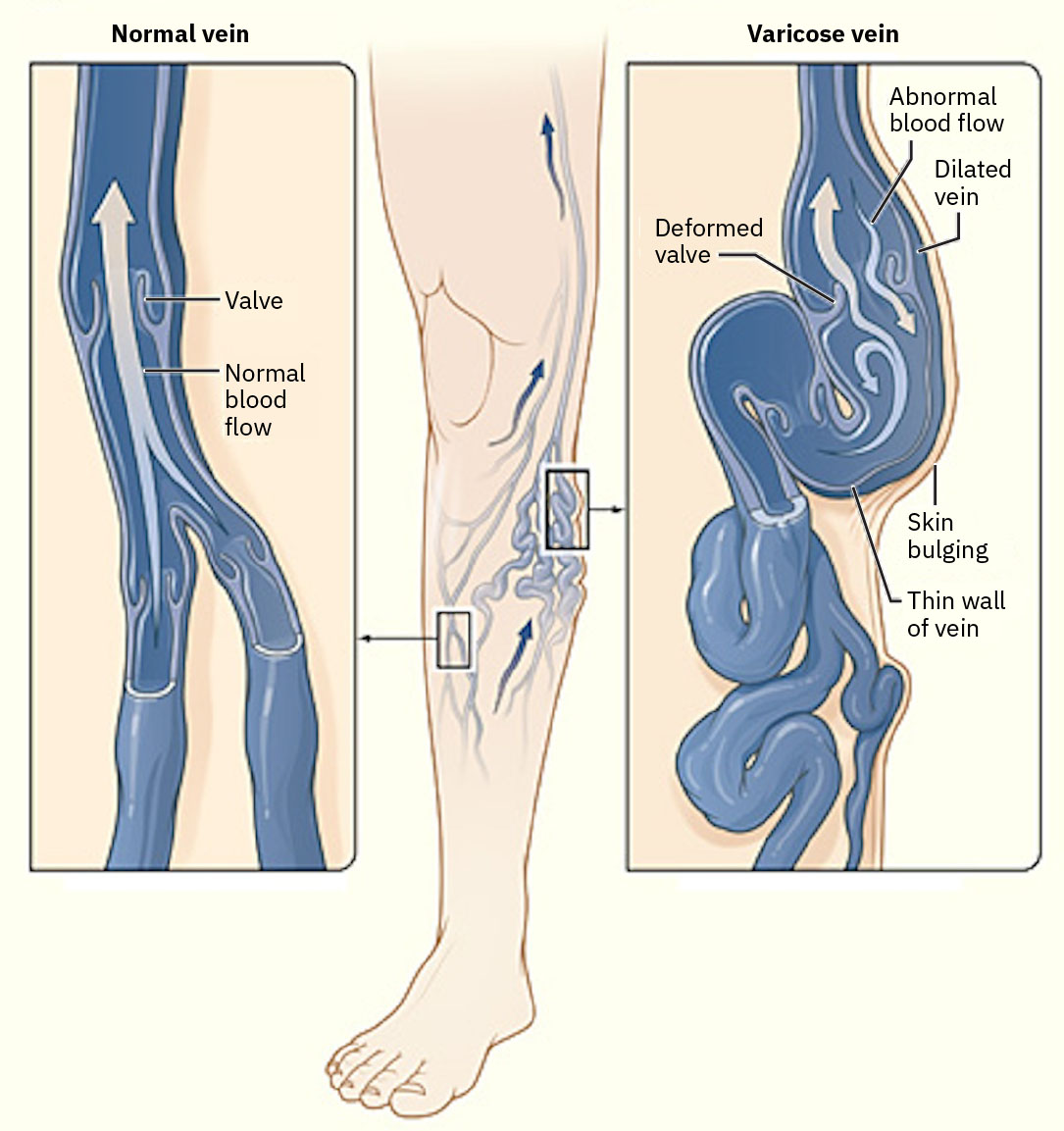 Illustration reference: OpenStax Medical-Surgical Nursing Ch.12.7.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.12.7.
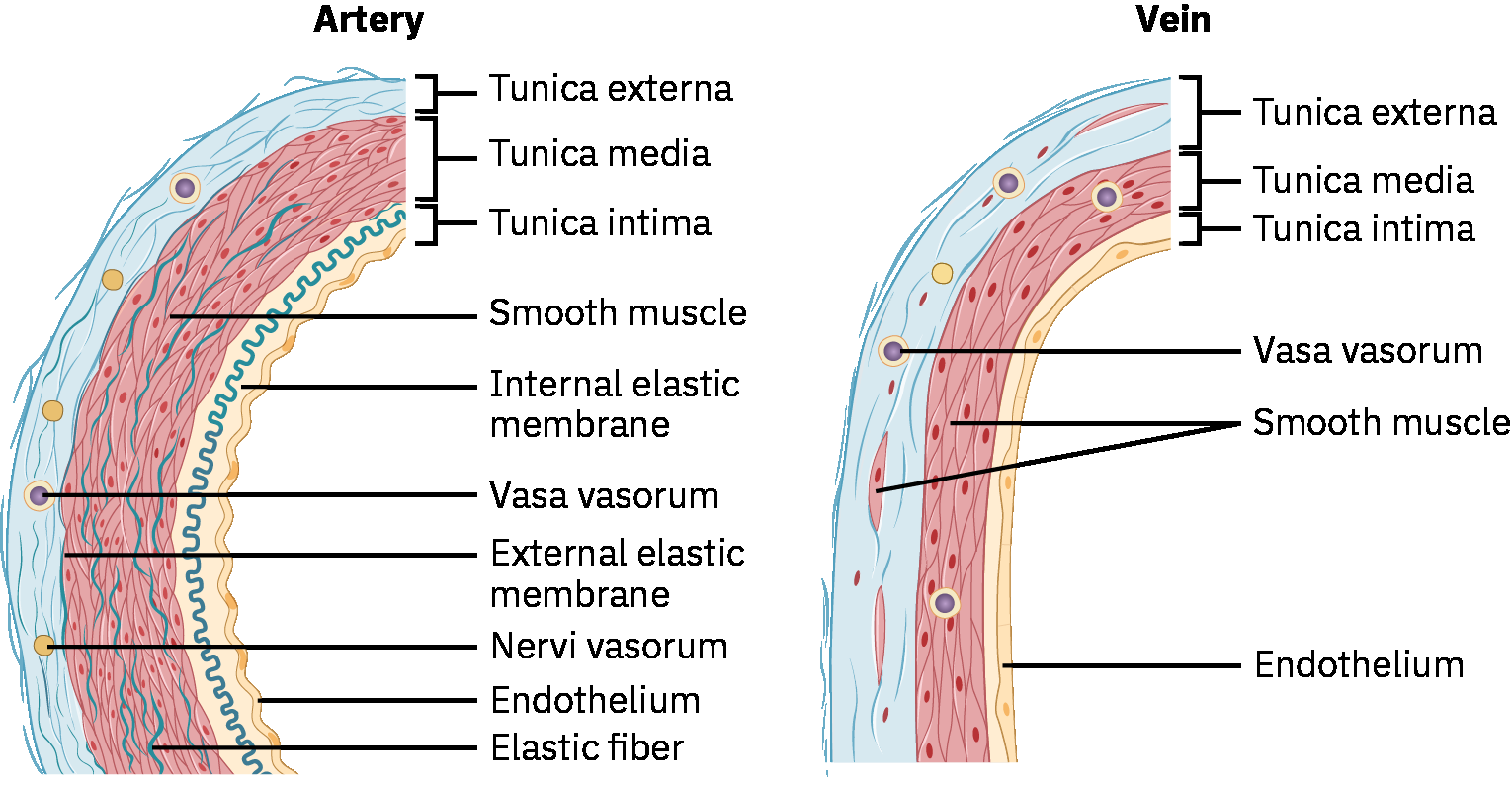 Illustration reference: OpenStax Pharmacology Ch.18.1.
Illustration reference: OpenStax Pharmacology Ch.18.1.
Nagbibigay ang venules ng transisyon mula capillary exchange patungo sa venous return. Ang postcapillary venules ay lubhang reaktibo sa inflammation at nagpapahintulot ng paglabas ng plasma proteins at leukocytes sa panahon ng inflammatory o infectious responses.
Mahalagang exception sa karaniwang oxygen-content patterns ang pulmonary circulation: ang pulmonary artery ay nagdadala ng deoxygenated blood patungo sa baga, at ibinabalik ng pulmonary veins ang oxygenated blood sa puso.
Classification
- Vessel classes: Arteries/arterioles para sa pasulong na oxygenated flow, capillaries para sa exchange, at venules/veins para sa return flow.
- Disorder classes: Occlusive disorders kumpara sa functional vascular disorders.
- Insufficiency pattern classes: Arterial insufficiency at venous insufficiency.
- Common occlusive examples: Atherosclerosis, Buerger disease, carotid artery disease, DVT, at lymphedema-related outflow obstruction patterns.
- Common functional examples: Chronic venous insufficiency, Raynaud phenomenon, at varicose veins.
- Common peripheral-assessment disorder groups: Venous stasis dermatitis, vasculitis, PAD, at mixed venous-arterial insufficiency.
Pagtatasa sa Nursing
Pokus sa NCLEX
Ihambing ang bilateral lower-extremity findings at i-trend ang exertional pain patterns sa halip na umasa sa iisang isolated cue.
- Tayahin ang exertional calf/thigh/buttock pain na humuhupa sa pahinga (intermittent claudication pattern).
- Tayahin ang temperature, color, edema distribution, skin texture, at ulcer location patterns.
- Tayahin ang mas malawak na peripheral abnormality clusters kabilang ang edema, cellulitis-like changes, temperature asymmetry, color change, reduced pulses, at ulceration.
- Kung kasabay ng peripheral findings ang systemic inflammatory symptoms (fatigue, fever, diffuse aches, appetite/weight loss), isaalang-alang ang vasculitis-pattern escalation.
- Tayahin ang peripheral pulse quality at symmetry na may focused attention sa diminished unilateral findings.
- Tayahin ang acute severe ischemia gamit ang 6 P findings at mag-escalate nang mabilis kapag present.
- Tayahin ang bagong exertional unilateral calf/thigh/buttock pain na humuhupa sa pahinga bilang claudication-pattern ischemia at i-trend ang severity/distance-to-onset sa paglipas ng panahon.
- Linawin kung ang exertional leg pain ay intermittent at humuhupa sa pahinga kumpara sa persistent pain kahit nagpapahinga, dahil ang pag-usad tungo sa rest pain ay nagpapahiwatig ng lumalalang ischemia.
- Tayahin ang risk factors tulad ng smoking history, hypertension, dyslipidemia, systemic inflammation, older age, diabetes, prior arterial injury/trauma, at activity limitation.
- Isama ang lifestyle-pattern screening para sa tobacco exposure, saturated-fat dominant diet, at physical inactivity dahil pinapabilis ng mga ito ang plaque-mediated vascular progression.
- Tayahin ang venous-insufficiency contributors tulad ng prior DVT, varicose veins, obesity, pregnancy history, at prolonged sitting o standing exposure.
- Tayahin ang cross-system manifestations ng reduced perfusion, kabilang ang angina, TIA/stroke-like symptoms, reduced urine output, delayed wound healing, at vision changes.
- Tayahin ang trophic skin changes tulad ng hair loss sa lower extremities, brittle o thickened nails, at nonhealing toe/foot ulcers.
- Tayahin ang arterial-insufficiency findings kabilang ang cool temperature, pale color, exertional pain, at ischemic-ulcer patterns; bantayang mabuti ang black necrotic tissue bilang limb-threat cue.
- Tayahin ang arterial skin-color pattern changes (pallor sa elevation at dusky/red dependent color) at capillary refill na delayed nang lampas tatlong segundo.
- Tayahin ang venous-pattern findings kabilang ang progressive ankle/lower-leg edema, leg heaviness o aching, pangangati, dark/discolored skin, thick brown stasis changes, dry o scaly texture, tortuous superficial veins, at pagbuo ng weeping venous ulcers sa severe disease.
- Karaniwang lumalala ang venous-insufficiency discomfort sa prolonged standing at maaaring gumaan sa rest/elevation; isama ang positional pattern na ito sa symptom triage.
- Sa chronic venous disease, idokumento ang nail changes (halimbawa thickened, discolored, o raised nail-bed appearance) kasabay ng skin/hair findings.
- I-differentiate ang thermal patterns: ang cold/clammy lower-extremity skin ay sumusuporta sa arterial insufficiency, samantalang ang warm ankles na may edema ay sumusuporta sa venous insufficiency.
- I-differentiate ang ulcer patterns: ang arterial ulcers ay kadalasang masakit, distal (toes/feet), round/smooth, dry o black-eschar dominant, at kaugnay ng weak/absent pulses; ang venous ulcers ay kadalasang nasa medial-ankle/low-leg, irregular na may drainage/slough, at kaugnay ng edema at preserved pulses.
- Sa lower-leg ulcer triage, tandaan ang location cues: kadalasang nagkakluster ang venous ulcers sa medial calf/ankle “gaiter area,” habang mas karaniwan ang arterial ulcers sa toes/ankle pressure points.
- Karaniwang lumilitaw ang venous-stasis ulcers sa medial o lateral distal lower-leg regions at maaaring mababaw, irregular, brown-yellow periwound lesions na minimally painful.
- Ang yellow periwound tissue sa venous-ulcer beds ay maaaring magpahiwatig ng necrotic/slough burden at dapat i-track sa wound-status documentation.
- I-map ang pain location sa malamang arterial territory kung posible (halimbawa thigh/buttock/aortoiliac distribution, calf/femoropopliteal distribution, foot/tibial-peroneal distribution).
- Ituring ang edema bilang senyales sa halip na standalone diagnosis; ang asymmetric unilateral edema ay dapat magtaas ng pag-aalala para sa local venous thrombosis.
Diagnostic Testing Cues
- I-review ang lipid profile at inflammatory markers (halimbawa C-reactive protein) sa pangkalahatang atherosclerotic-risk interpretation.
- Asahan ang Doppler ultrasound upang matukoy ang arterial narrowing at flow reduction sa apektadong limbs.
- Asahan ang segmental pressure measurements upang i-localize ang arterial narrowing sa pamamagitan ng paghahambing ng pressures sa thigh, calf, at ankle levels.
- Asahan ang ankle-brachial index (ABI) testing; ang mas mababang ABI values ay sumusuporta sa reduced lower-extremity arterial perfusion.
- Maaaring ihambing ng exercise ABI protocols ang arm-leg pressures sa pahinga at pagkatapos ng graded treadmill walking; ang postactivity pressure decline kasama ang claudication symptoms ay sumusuporta sa flow-limitation diagnosis.
- Asahan ang carotid ultrasound kapag pinaghihinalaan ang carotid flow limitation.
- Sa carotid-disease pathways, ang duplex velocity findings na may stenosis na higit sa humigit-kumulang 50% ay madalas mag-trigger ng pharmacologic o procedural treatment planning.
- Ang carotid stenosis na mas mababa sa humigit-kumulang 50% ay kadalasang mina-manage sa medical monitoring, habang ang higher-grade disease ay sinusuri para sa revascularization candidacy.
- Asahan ang coronary angiography o coronary CT angiography kapag kinakailangan ang coronary plaque burden/stricture assessment.
- Asahan ang venous Doppler/ultrasound flow studies upang suriin ang venous directionality at reflux patterns; asahan ang venography na may contrast kapag kailangan ng mas detalyadong localization ng restricted venous segments.
- Asahan ang ankle-brachial index (ABI) workflow na naghahambing ng brachial pressure sa dorsalis pedis/posterior tibial ankle pressures; ang accuracy ay nakadepende sa tamang cuff/probe technique.
- Para sa disease-burden stratification, i-trend ang lipid elevation at hemoglobin A1C patterns dahil karaniwang magkakasabay ang hyperlipidemia at diabetes burden sa PAD/PVD progression.
Mga Interbensyon sa Nursing
- Agad i-escalate ang mga senyales ng acute ischemic o thromboembolic concern.
- Palakasin ang risk-factor modification kabilang ang tobacco cessation, activity progression, at follow-up adherence.
- Gumamit ng structured secondary-prevention targets kapag inutos sa advanced vascular disease (halimbawa LDL na mas mababa sa humigit-kumulang 70 mg/dL, A1C na mas mababa sa humigit-kumulang 7%, at controlled blood-pressure trends).
- Ituro ang prescribed walking therapy progression (lumakad hanggang pain threshold, magpahinga, pagkatapos ay magpatuloy) upang suportahan ang pagbuo ng collateral circulation.
- I-coordinate ang inutusang vascular diagnostics at structured reassessment para sa symptom progression.
- Palakasin ang heart-healthy nutrition, blood-pressure control, lipid management, weight optimization, at diabetes blood-glucose control.
- Ituro sa mga pasyente kung aling bago o lumalalang sintomas ang nangangailangan ng agarang provider notification.
- Ituro ang limb-protection strategies: iwasan ang constrictive clothing at leg crossing; gabayan ang leg positioning batay sa perfusion at edema status (kabilang ang dependent positioning para sa arterial flow support at pag-iwas sa elevation above heart level kapag magkasabay ang edema/perfusion concerns).
- Palakasin ang daily foot at skin inspection na may agarang pag-report ng injury o nonhealing breakdown.
- Pagkatapos ng revascularization procedures, i-monitor ang surgical site integrity at distal pulses; agad i-report ang decreased perfusion, posibleng bypass compromise, o pinaghihinalaang bypass rupture.
- Sa carotid disease pathways, karaniwang kabilang sa CEA candidacy ang symptomatic stenosis na humigit-kumulang 50-99% at piling asymptomatic severe stenosis na humigit-kumulang 70-99% ayon sa vascular-team criteria.
- Palakasin ang venous-return strategies: consistent use ng correctly fitted graduated compression stockings, scheduled leg elevation above heart level, calf-muscle activation exercises, at pag-iwas sa prolonged immobility.
- Para sa pinaghihinalaang arterial-ulcer patterns, iwasan ang compression hanggang makumpirma ng ABI o katumbas na perfusion testing ang ligtas na arterial inflow.
- Para sa chronic venous insufficiency, turuan ang madalas na position changes at pag-iwas sa prolonged standing; kapag lumalala ang swelling, palakasin ang pillow-supported leg elevation at hydration upang mabawasan ang pooling risk.
- I-coordinate ang evaluation para sa procedural venous interventions (halimbawa, sclerotherapy o vein ligation/stripping) kapag hindi sapat ang conservative symptom-control measures.
- Sa painful varicose-vein disease sa kabila ng conservative care, mag-escalate para sa wound-care o vascular-specialist referral at talakayin ang procedural options (halimbawa venous stripping) ayon sa team plan.
- Para sa venous stasis dermatitis patterns, palakasin ang limb elevation, progressive muscle activation, at prescribed static/stocking compression plans habang dini-differentiate ang chronic stasis change mula sa acute bacterial cellulitis.
- Para sa PAD patterns, palakasin ang supervised exercise progression, smoking cessation, lipid/risk-factor control, wound-care adherence, at routine foot inspection.
- Sa symptomatic claudication phases, i-pace ang ambulation ayon sa individual tolerance at iwasan ang prolonged overexertion habang pinananatili ang structured walking-program goals.
- Para sa arterial-ulcer care, i-coordinate ang inutusang wound dressings at debridement pathways at i-monitor ang pag-usad ng impeksiyon.
- Sa mixed venous-arterial insufficiency, gumamit ng ABI-guided planning, mag-monitor nang mabuti para sa wound infection, at i-coordinate ang revascularization/wound-specialist pathways ayon sa utos.
- Sa severe arterial insufficiency na hindi nakokontrol sa medikal na paraan, asahan ang angiography na maaaring may kasamang endovascular repair o arterial-bypass referral.
Pag-usad na Nagbabanta sa Limb
Ang hindi nagamot na progressive insufficiency ay maaaring humantong sa critical ischemia, tissue necrosis, debridement/amputation requirement, at pagkawala ng limb function.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| coronary-artery-disease(sakit sa coronary artery - antilipemics) | Statin therapy contexts | Pinabababa ang LDL burden at binabawasan ang panganib ng plaque progression. |
| antiplatelets(mga antiplatelet) | Aspirin-class therapy contexts | Binabawasan ang thrombosis risk sa atherosclerotic arterial disease. |
| antihypertensives(mga antihypertensive) | Blood-pressure control contexts | Binabawasan ang arterial strain at downstream ischemic complications. |
| anticoagulants(mga anticoagulant) | Anticoagulant therapy contexts | Gumamit ng focused bleeding surveillance at i-monitor ang perfusion changes. |
| vasodilators | Vasodilator therapy contexts | I-monitor ang blood pressure response at symptom relief kasama ang perfusion trends. |
| cholesterol absorption inhibitors | Ezetimibe-class contexts | Sumusuporta sa karagdagang lipid reduction kapag hindi naaabot ang LDL targets. |
| thrombolytic therapy | Acute limb clot contexts | Ireserba para sa acute obstruction protocols na may mahigpit na bleeding at perfusion monitoring. |
Paglalapat ng Clinical Judgment
Klinikal na Sitwasyon
Isang pasyente ang nag-uulat ng calf cramping matapos ang maikling distansya ng paglalakad na humuhupa sa pahinga; mas mahina at mas malamig ang right foot pulse kumpara sa kaliwa.
- Recognize Cues: Exertional unilateral pain na may pulse at temperature asymmetry.
- Analyze Cues: Ang pattern ay tugma sa peripheral arterial insufficiency.
- Prioritize Hypotheses: Pinakamataas na prayoridad ang pagpigil sa pag-usad tungo sa critical ischemia.
- Generate Solutions: Simulan ang focused vascular follow-up at palakasin ang risk-reduction plan.
- Take Action: I-escalate ang findings at malinaw na idokumento ang bilateral comparison.
- Evaluate Outcomes: Nasisimulan nang walang delay ang diagnostic workup at treatment plan, at hindi umuusad ang symptom progression tungo sa critical limb ischemia.
Mga Kaugnay na Konsepto
- cardiovascular system - Mahigpit na magkaugnay ang central cardiac function at peripheral flow.
- impaired skin and tissue integrity - Inuugnay ang perfusion-pattern findings sa tissue-injury at healing consequences.
- hypertension assessment and management - Madalas na nagsasapawan ang chronic pressure burden at vascular injury progression.
- capillary filtration - Tinutukoy ng microvascular exchange ang tissue-level delivery at clearance.
- fluid volume overload (hypervolemia) - Nakaaapekto ang volume status sa edema burden at vascular findings.
- pagtatasa sa nursing ng cardiovascular at peripheral vascular - Assessment sequence at escalation thresholds para sa bedside care.
Sariling Pagsusuri
- Aling mga katangian ang pinakamahusay na naghihiwalay sa arterial mula sa venous insufficiency sa bedside?
- Bakit mahalaga ang bilateral pulse at skin comparison sa peripheral vascular assessment?
- Kailan dapat mag-trigger ang intermittent claudication symptoms ng agarang follow-up escalation?